Progress Toward Regional Measles Elimination — Worldwide, 2000–2014Robert T. Perry, MD1; Jillian S. Murray, MSPH1; Marta Gacic-Dobo, MSc1; Alya Dabbagh, PhD1; Mick N. Mulders, PhD1; Peter M. Strebel, MBChB1; Jean-Marie Okwo-Bele, MD1; Paul A. Rota, PhD2; James L. Goodson, MPH3 In 2000, the United Nations General Assembly adopted the Millennium Development Goals (MDG), with MDG4 being a two-thirds reduction in child mortality by 2015, and with measles vaccination coverage being one of the three indicators of progress toward this goal.* In 2010, the World Health Assembly established three milestones for measles control by 2015: 1) increase routine coverage with the first dose of measles-containing vaccine (MCV1) for children aged 1 year to =90% nationally and =80% in every district; 2) reduce global annual measles incidence to fewer than five cases per million population; and 3) reduce global measles mortality by 95% from the 2000 estimate (1).† In 2012, the World Health Assembly endorsed the Global Vaccine Action Plan§ with the objective to eliminate measles in four World Health Organization (WHO) regions by 2015. WHO member states in all six WHO regions have adopted measles elimination goals. This report updates the 2000–2013 report (2) and describes progress toward global control and regional measles elimination during 2000–2014. During this period, annual reported measles incidence declined 73% worldwide, from 146 to 40 cases per million population, and annual estimated measles deaths declined 79%, from 546,800 to 114,900. However, progress toward the 2015 milestones and elimination goals has slowed markedly since 2010. To resume progress toward milestones and goals for measles elimination, a review of current strategies and challenges to improving program performance is needed, and countries and their partners need to raise the visibility of measles elimination, address barriers to measles vaccination, and make substantial and sustained additional investments in strengthening health systems. Immunization ActivitiesTo estimate coverage with MCV1 and the second dose of MCV (MCV2) through routine immunization services,¶ WHO and the United Nations Children's Fund (UNICEF) use data from administrative records and surveys reported annually by the 194 WHO countries. From 2000 to 2010, estimated MCV1 coverage increased globally from 72% to 85%, and remained at 85% through 2014 (Tables 1 and 2). The number of countries with =90% MCV1 coverage increased from 84 (44%) in 2000 to 131 (68%) in 2012, then decreased to 122 (63%) in 2014. Since 2003, countries also have reported the number of districts with =80% MCV1 coverage. Among countries with =90% MCV1 coverage nationally, the percentage having =80% MCV1 coverage in all districts increased from 1% (1 of 103) in 2003 to 44% (57 of 131) in 2012, then declined to 40% (49 of 122) in 2014. Among the estimated 20.6 million infants who did not receive MCV1 through routine immunization services in 2014, approximately 11.6 million (56%) were in six countries: the Democratic Republic of the Congo (0.6 million), Ethiopia (0.9 million), India (4.2 million), Indonesia (1 million), Nigeria (3.3 million), and Pakistan (1.6 million). During 2000–2014, the number of countries providing MCV2 nationally through routine immunization services increased from 97 (51%) to 154 (79%), with six countries (Burkina Faso, Morocco, Niger, Rwanda, Senegal, Tanzania) introducing MCV2 in 2014. Estimated global MCV2 coverage increased from 15% in 2000 to 56% in 2014. During 2014, approximately 221 million children received MCV during mass immunization campaigns known as supplementary immunization activities (SIAs)** conducted in 29 countries, with 23 countries (79%) providing one or more additional child health interventions during the SIA (Figure). Based on doses administered, SIA coverage was =95% in 16 (55%) countries; however, of the five countries conducting post-SIA coverage surveys, only one estimated SIA coverage at =95%. Disease IncidenceCountries report the number of measles cases from either case-based or aggregate surveillance systems†† to WHO and UNICEF each year. Effective measles surveillance includes case-based surveillance with laboratory testing to confirm cases. In 2014, 187 (96%)§§ countries used case-based surveillance, and 191 (98%)¶¶ had access to standardized quality-controlled testing through the WHO Global Measles and Rubella Laboratory Network. During 2000–2014, the number of annually reported measles cases worldwide decreased 69%, from 853,479 to 267,482, and measles incidence decreased 73%, from 146 to 40 cases per million population (Tables 1 and 2). The results for 2014 represent little change from those reported in 2013 (280,795 cases and 40 cases per million population), although fewer countries reported in 2014 (169) compared with 2013 (175).*** The percentage of reporting countries with <5 cases per million decreased from 65% (113 of 175) in 2013 to 58% (98 of 169) in 2014. During 2000–2014, the Region of the Americas (AMR) maintained measles incidence at fewer than 5 cases per million. Measles incidence decreased in four of six WHO regions from 2013 to 2014 (Table 2). In the African Region (AFR), reported cases decreased 57%, from 171,178 cases in 2013 to 73,914 in 2014, largely because of decreases in the Democratic Republic of the Congo (from 88,381 to 33,711) and Nigeria (from 52,852 to 6,855). However, in 2014, outbreaks occurred in Angola (11,699) and Ethiopia (12,739 cases). In the Eastern Mediterranean Region (EMR), the European Region (EUR), and the South-East Asia Region (SEAR), reported cases also decreased in 2014, although large outbreaks were reported in India (24,977), Somalia (10,278 cases), and Russia (4,711) in 2014. Increased numbers of cases were reported in 2014 from AMR, largely because of outbreaks in Brazil (727 cases) and the United States (667); and from the Western Pacific Region (WPR), because of large outbreaks reported in China (52,628), the Philippines (58,848 cases), and Vietnam (15,033). Genotypes of viruses isolated from measles cases were reported to WHO by 69 (41%) of the 169 countries reporting measles cases in 2014. Of the 24 recognized measles virus genotypes, 11 were detected during 2005–2008 and eight during 2009–2014, excluding those from vaccine reactions and cases of subacute sclerosing panencephalitis (3). In 2014, among 7,155 reported sequences,††† 1,328 (50 countries) were genotype B3, 38 (eight countries) were D4, 1,083 (45 countries) were D8, 92 (12 countries) were D9, four (four countries) were G3, and 4,610 (18 countries) were H1 (Table 2). Mortality EstimatesWHO has developed a model to estimate measles mortality in countries using numbers and age distribution of reported cases, routine and SIA MCV coverage, and age- and country-specific case-fatality ratios (4,5). New measles vaccination coverage and case data for all countries during 2000–2014 led to a new series of mortality estimates. During this period, estimated measles deaths decreased 79%, from 546,800 to 114,900, and all regions had substantial reductions in estimated measles mortality (Tables 1 and 2). Compared with no measles vaccination, measles vaccination prevented an estimated 17.1 million deaths during 2000–2014 (Figure). Regional Verification of Measles EliminationSince the last report, the AMR regional verification committee determined that AMR cannot be declared measles free, because Brazil has had sustained transmission of a single measles virus strain for >1 year. The WPR regional verification committee verified absence of endemic measles in two member states and one area, bringing the total to seven in WPR (6); the EUR regional verification committee verified measles elimination in 22 member states (7). DiscussionDuring 2000–2014, increased coverage worldwide with both (1st and 2nd) routine doses of MCV, combined with SIAs in countries that lack high coverage with 2 doses of MCV, contributed to a 73% decrease in reported measles incidence and a 79% reduction in estimated measles mortality. During this period, measles vaccination prevented an estimated 17.1 million deaths. However, on the basis of current trends in measles vaccination coverage and incidence, the WHO Strategic Advisory Group of Experts on Immunization concluded that the 2015 global milestones and measles elimination goals will not be achieved (8). Measles can serve as an indicator of the strength and reach of the health system, as measles outbreaks reveal populations poorly served by health services. In high-burden, low-coverage countries, outbreak investigations have also found low MCV1 coverage where long-standing policies and practices prevent vaccination of children aged =12 months, discourage opening a 10-dose vial when few children are present, and limit measles vaccination to only one session per month (Global Immunization Division, Center for Global Health, CDC, unpublished data, 2015). Addressing these gaps, maximizing how SIA planning and implementation can improve routine services, and conducting high-quality SIAs should increase coverage and equity for all vaccines and further reduce the number of measles cases and deaths. As coverage improves, establishing a visit during the second year of life integrating MCV2 and other child health interventions should help to further reduce measles burden. The findings in this report are subject to at least three limitations. First, MCV coverage estimates are affected by inclusion of SIA doses administered to children outside the target group, inaccurate estimates of the target population size, and inaccurate reports of the number of doses delivered. Second, under-ascertainment of measles cases through surveillance systems can occur, because not all patients with measles seek care and not all cases are reported. Third, some countries report aggregate numbers of unconfirmed cases rather than case-based data. The decrease in measles mortality is among three main contributors (along with decreases in pneumonia and diarrhea) to the decline in overall child mortality and progress toward MDG4 (9). To assess the reasons for the slowing of progress since 2010 and to modify current strategies as needed, the Measles & Rubella Initiative§§§ partners have commissioned a midterm strategy review. Countries and their partners need to raise the visibility of measles elimination, and secure the resources needed to implement strategies required to reach measles control and elimination goals, taking into account the results and recommendations from the review. 1Department of Immunization, Vaccines, and Biologicals, World Health Organization; 2Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC; 3Global Immunization Division, Center for Global Health, CDC. Corresponding author: James L. Goodson, jgoodson@cdc.gov, 404-639-8170. References
* Additional information available at http://www.unmillenniumproject.org/goals/gti.htm#goal4. † Whereas the coverage milestone is to be met by every country, the incidence and mortality reduction milestones are to be met globally. § The Global Vaccine Action Plan is the implementation plan of the Decade of Vaccines, a collaboration between WHO, UNICEF, the Bill and Melinda Gates Foundation, Gavi, the Vaccine Alliance, the U.S. National Institute of Allergy and Infectious Diseases, the African Leaders Malaria Alliance, and others to extend the full benefit of immunization to all persons by 2020 and beyond. Additional information is available at http://www.who.int/immunization/global_vaccine_action_plan and at http://apps.who.int/gb/ebwha/pdf_files/wha65/a65_22-en.pdf. ¶ For MCV1, among children aged 1 year or, if MCV1 is given at age =1 year, among children aged 24 months. For MCV2, among children at the recommended age of administration of MCV2, as per the national immunization schedule. WHO/UNICEF estimates of national immunization coverage are available at http://www.who.int/immunization/monitoring_surveillance/data. ** Supplemental immunization activities (SIAs) generally are carried out using two target age ranges. An initial, nationwide catch-up SIA focuses on all children aged 9 months–14 years, with the goal of eliminating susceptibility to measles in the general population. Periodic follow-up SIAs then focus on all children born since the last SIA. Follow-up SIAs generally are conducted nationwide every 2–4 years and focus on children aged 9–59 months; their goal is to eliminate any measles susceptibility that has developed in recent birth cohorts and to protect children who did not respond to MCV1. †† Available at http://apps.who.int/immunization_monitoring/globalsummary/timeseries/tsincidencemeasles.html. §§ Countries without case-based measles surveillance in 2014 were Djibouti, India, Mauritius, Sao Tome and Principe, Seychelles, Somalia, and South Sudan. ¶¶ Countries without access to standardized quality-controlled testing by the WHO Measles and Rubella Laboratory Network in 2014 were Cape Verde, Sao Tome and Principe, and Seychelles. *** Countries not reporting in 2013 were Cuba (AMR); Bahrain, Libya, and the United Arab Emirates (EMR); Austria, Bosnia and Herzegovina, Italy, Malta, Monaco, San Marino, and Ukraine (EUR); and Brunei Darussalam, Cook Islands, Fiji, the Marshall Islands, Nauru, Samoa, Singapore, and Tuvalu (WPR). In 2014, countries not reporting were Djibouti and Oman (EMR); Albania, Andorra, Croatia, Finland, Italy, Luxembourg, Monaco, Montenegro, Poland, San Marino, and Ukraine (EUR); Indonesia and Thailand (SEAR); and Cook Islands, Fiji, Marshall Islands, Nauru, Niue, Singapore, Solomon Islands, Tonga, Tuvalu, and Western Samoa (WPR). ††† Sequences were for the 450 nucleotide carboxy-terminal of the nucleocapsid gene in the measles virus genome. Genotypes isolated from three cases of subacute sclerosing panencephalitis (D3, D6, and D7) were excluded from the total. Data (as of October 7, 2015) available from the Measles Nucleotide Surveillance (MeaNS) database, available at http://www.who-measles.org/Public/Web_Front/main.php. §§§ The Measles & Rubella Initiative is a partnership established in 2001 as the Measles Initiative, led by the American Red Cross, CDC, the United Nations Foundation, UNICEF, and WHO. Additional information is available at http://www.measlesrubellainitiative.org. Summary What is already known on this topic? During 2000–2010, global vaccination coverage with the 1st dose of measles-containing vaccine (MCV1) increased from 72% to 85%, and annual measles incidence decreased from 146 reported cases per million population in 2000 to 50 cases per million in 2010. During 2010–2013, MCV1 coverage and measles incidence did not significantly change. What is added by this report? During 2000–2014, an estimated 17.1 million deaths were prevented by measles vaccination, and measles incidence decreased 73%, from 146 to 40 cases per million population. The number of countries providing the 2nd dose of measles-containing vaccine (MCV2) nationally through routine immunization services increased to 154 (79%) in 2014, and global MCV2 coverage was 56%. During 2014, a total of 221 million children were vaccinated against measles during supplementary immunization activities. What are the implications for public health practice? Although measles vaccination has saved millions of lives since 2000, progress has slowed since 2010. Reaching measles control and elimination goals will require addressing policy and practice gaps that prevent reaching larger numbers of children with measles vaccination, increasing visibility of measles elimination efforts, and ensuring adequate resources for strengthening health systems.
FIGURE. Estimated number of measles deaths and number of deaths averted by measles vaccination — worldwide, 2000–2014 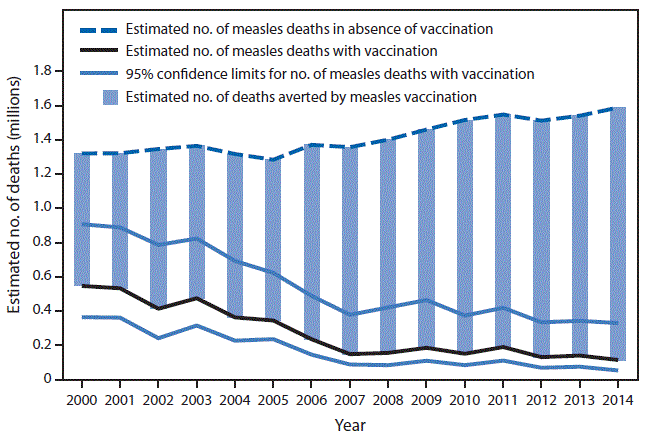
Alternate Text: The figure is a combination line and bar chart showing the estimated number of measles deaths and number of deaths averted by measles vaccination worldwide during 2000-2014. Syndicated Content Details:
Source URL: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6444a4.htm Source Agency: Centers for Disease Control and Prevention (CDC) Captured Date: 2016-05-23 23:13:30.0
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||