The marks in this booklet show actions you can take to manage your diabetes.
Help your health care team make a diabetes care plan that will work for you.
Learn to make wise choices for your diabetes care each day.
Step 1: Learn about diabetes.
What is diabetes?
There are three main types of diabetes:
Type 1 diabetes – Your body does not make insulin. This is a problem because you need insulin to take the sugar (glucose) from the foods you eat and turn it into energy for your body. You need to take insulin every day to live.
Type 2 diabetes – Your body does not make or use insulin well. You may need to take pills or insulin to help control your diabetes. Type 2 is the most common type of diabetes.
Gestational (jest-TAY-shun-al) diabetes – Some women get this kind of diabetes when they are pregnant. Most of the time, it goes away after the baby is born. But even if it goes away, these women and their children have a greater chance of getting diabetes later in life.
You are the most important member of your health care team.
You are the one who manages your diabetes day by day. Talk to your doctor about how you can best care for your diabetes to stay healthy. Some others who can help are:
dentist
diabetes doctor
diabetes educator
dietitian
eye doctor
foot doctor
friends and family
mental health counselor
nurse
nurse practitioner
pharmacist
social worker
How to learn more about diabetes.
Take classes to learn more about living with diabetes. To find a class, check with your health care team, hospital, or area health clinic. You can also search online.
Join a support group — in-person or online — to get peer support with managing your diabetes.
You may have heard people say they have “a touch of diabetes” or that their “sugar is a little high.” These words suggest that diabetes is not a serious disease. That is not correct. Diabetes is serious, but you can learn to manage it.
People with diabetes need to make healthy food choices, stay at a healthy weight, move more every day, and take their medicine even when they feel good. It’s a lot to do. It’s not easy, but it’s worth it!
Why take care of your diabetes?
Taking care of yourself and your diabetes can help you feel good today and in the future. When your blood sugar (glucose) is close to normal, you are likely to:
have more energy
be less tired and thirsty
need to pass urine less often
heal better
have fewer skin or bladder infections
You will also have less chance of having health problems caused by diabetes such as:
heart attack or stroke
eye problems that can lead to trouble seeing or going blind
pain, tingling, or numbness in your hands and feet, also called nerve damage
kidney problems that can cause your kidneys to stop working
teeth and gum problems
Actions you can take
Ask your health care team what type of diabetes you have.
Learn where you can go for support.
Learn how caring for your diabetes helps you feel good today and in the future.
Step 2: Know your diabetes ABCs.
Talk to your health care team about how to manage your A1C, Blood pressure, and Cholesterol. This can help lower your chances of having a heart attack, stroke, or other diabetes problems.
A for the A1C test (A-one-C).
What is it?
The A1C is a blood test that measures your average blood sugar level over the past three months. It is different from the blood sugar checks you do each day.
Why is it important?
You need to know your blood sugar levels over time. You don’t want those numbers to get too high. High levels of blood sugar can harm your heart, blood vessels, kidneys, feet, and eyes.
What is the A1C goal?
The A1C goal for many people with diabetes is below 7. It may be different for you. Ask what your goal should be.
B for Blood pressure.
What is it?
Blood pressure is the force of your blood against the wall of your blood vessels.
Why is it important?
If your blood pressure gets too high, it makes your heart work too hard. It can cause a heart attack, stroke, and damage your kidneys and eyes.
What is the blood pressure goal?
The blood pressure goal for most people with diabetes is below 140/90. It may be different for you. Ask what your goal should be.
C for Cholesterol (ko-LESS-tuh-ruhl).
What is it?
There are two kinds of cholesterol in your blood: LDL and HDL.
LDL or “bad” cholesterol can build up and clog your blood vessels. It can cause a heart attack or stroke.
HDL or “good” cholesterol helps remove the “bad” cholesterol from your blood vessels.
What are the LDL and HDL goals?
Ask what your cholesterol numbers should be. Your goals may be different from other people. If you are over 40 years of age, you may need to take a statin drug for heart health.
Actions you can take
Ask your health care team:
what your A1C, blood pressure, and cholesterol numbers are and what they should be. Your ABC goals will depend on how long you have had diabetes, other health problems, and how hard your diabetes is to manage.
what you can do to reach your ABC goals
Write down your numbers on the record at the back of this booklet to track your progress.
Step 3: Learn how to live with diabetes.
It is common to feel overwhelmed, sad, or angry when you are living with diabetes. You may know the steps you should take to stay healthy, but have trouble sticking with your plan over time. This section has tips on how to cope with your diabetes, eat well, and be active.
Cope with your diabetes.
Stress can raise your blood sugar. Learn ways to lower your stress. Try deep breathing, gardening, taking a walk, meditating, working on your hobby, or listening to your favorite music.
Ask for help if you feel down. A mental health counselor, support group, member of the clergy, friend, or family member who will listen to your concerns may help you feel better.
Eat well.
Make a diabetes meal plan with help from your health care team.
Choose foods that are lower in calories, saturated fat, trans fat, sugar, and salt.
Eat foods with more fiber, such as whole grain cereals, breads, crackers, rice, or pasta.
Choose foods such as fruits, vegetables, whole grains, bread and cereals, and low-fat or skim milk and cheese.
Drink water instead of juice and regular soda.
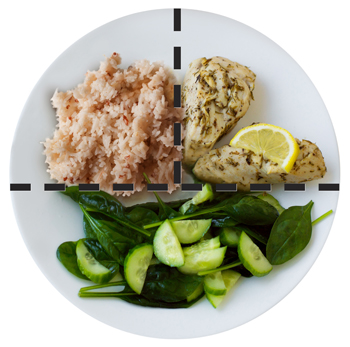
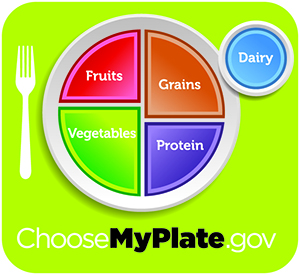
When eating a meal, fill half of your plate with fruits and vegetables, one quarter with a lean protein, such as beans, or chicken or turkey without the skin, and one quarter with a whole grain, such as brown rice or whole wheat pasta.
Be active.
Set a goal to be more active most days of the week. Start slow by taking 10 minute walks, 3 times a day.
Twice a week, work to increase your muscle strength. Use stretch bands, do yoga, heavy gardening (digging and planting with tools), or try push-ups.
Stay at or get to a healthy weight by using your meal plan and moving more.
Know what to do every day.
Take your medicines for diabetes and any other health problems even when you feel good. Ask your doctor if you need aspirin to prevent a heart attack or stroke. Tell your doctor if you cannot afford your medicines or if you have any side effects.
Check your feet every day for cuts, blisters, red spots, and swelling. Call your health care team right away about any sores that do not go away.
Brush your teeth and floss every day to keep your mouth, teeth, and gums healthy.
Stop smoking. Ask for help to quit. Call 1-800-QUITNOW (1-800-784-8669).
Keep track of your blood sugar. You may want to check it one or more times a day. Use the card at the back of this booklet to keep a record of your blood sugar numbers. Be sure to talk about it with your health care team.
Check your blood pressure if your doctor advises and keep a record of it.
Talk to your health care team.
Ask your doctor if you have any questions about your diabetes.
Report any changes in your health.
Actions you can take
Ask for a healthy meal plan.
Ask about ways to be more active.
Ask how and when to test your blood sugar and how to use the results to manage your diabetes.
Use these tips to help with your self-care.
Discuss how your diabetes plan is working for you each time you visit your health care team.
Step 4: Get routine care to stay healthy.
See your health care team at least twice a year to find and treat any problems early.
At each visit, be sure you have a:
blood pressure check
foot check
weight check
review of your self-care plan
Two times each year, have an:
A1C test. It may be checked more often if it is over 7.
Once each year, be sure you have a:
cholesterol test
complete foot exam
dental exam to check teeth and gums
dilated eye exam to check for eye problems
flu shot
urine and a blood test to check for kidney problems
At least once in your lifetime, get a:
pneumonia (nu-mo-nya) shot
hepatitis B (HEP-uh-TY-tiss) shot
Medicare and diabetes.
If you have Medicare, check to see how your plan covers diabetes care. Medicare covers some of the costs for:
diabetes education
diabetes supplies
diabetes medicine
visits with a dietitian
special shoes, if you need them
Actions you can take
Ask your health care team about these and other tests you may need. Ask what your results mean.
Write down the date and time of your next visit.
Use the card at the back of this booklet to keep a record of your diabetes care.
If you have Medicare, check your plan.
Things to Remember:
You are the most important member of your health care team.
Follow the four steps in this booklet to help you learn how to manage your diabetes.
Learn how to reach your diabetes ABC goals.
Ask your health care team for help.
My Diabetes Care Record: Page 1
How to use the record.
First read the shaded bar across the page. This tells you:
the name of the test or check-up
how often to get the test or check-up
what your personal goal is (for A1C, blood pressure, and cholesterol)
Then, write down the date and results for each test or check-up you get. Take this card with you on your health care visits. Show it to your health care team. Talk about your goals and how you are doing.
A1C – At least twice each year
My goal: ______
Date
Result
Blood Pressure (BP) – At each visit
My goal: ______
Date
Result
Cholesterol – Once each year
My goal: ______
Date
Result
My Diabetes Care Record: Page 2
How to use the record.
Use this page to write down the date and results of each test, exam, or shot.
Each Visit
Date
Result
Foot check
Review self-care plan
Weight check
Review medicines
Once a Year
Date
Result
Dental exam
Dilated eye exam
Complete foot exam
Flu shot
Kidney check
At Least Once
Date
Result
Pneumonia shot
Hepatitis B shot
Self Checks of Blood Sugar
How to use this card.
This card has three sections. Each section tells you when to check your blood sugar: before each meal, 1 to 2 hours after each meal, and at bedtime. Each time you check your blood sugar, write down the date, time, and results. Take this card with you on your health care visits. Show it to your health care team. Talk about your goals and how you are doing.
Date
Time
Result
My blood sugar before meals: Usual goal 80 to 130* My goal: ________
My blood sugar 1-2 hours after meals: Usual goal below 180* My goal: ________
My blood sugar at bedtime: Usual goal 110 to 150* My goal: ________
* Your blood sugar goals may be different if you are an older adult (over 65) and have had diabetes a long time. They may be different if you have other health problems like heart disease, or your blood sugar often gets too low.
The U.S. Department of Health and Human Services’ National Diabetes Education Program (NDEP) is jointly sponsored by the National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC) with the support of more than 200 partner organizations.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Carbohydrate counting, also called carb counting, is a meal planning tool for people with type 1 or type 2 diabetes. Carbohydrate counting involves keeping track of the amount of carbohydrate in the foods you eat each day.
Carbohydrates are one of the main nutrients found in food and drinks. Protein and fat are the other main nutrients. Carbohydrates include sugars, starches, and fiber. Carbohydrate counting can help you control your blood glucose, also called blood sugar, levels because carbohydrates affect your blood glucose more than other nutrients.
Healthy carbohydrates, such as whole grains, fruits, and vegetables, are an important part of a healthy eating plan because they can provide both energy and nutrients, such as vitamins and minerals, and fiber. Fiber can help you prevent constipation, lower your cholesterol levels, and control your weight.
Unhealthy carbohydrates are often food and drinks with added sugars. Although unhealthy carbohydrates can also provide energy, they have little to no nutrients. More information about which carbohydrates provide nutrients for good health and which carbohydrates do not is provided in the NIDDK health topic, Diabetes Diet and Eating.
The amount of carbohydrate in foods is measured in grams. To count grams of carbohydrate in foods you eat, you’ll need to
know which foods contain carbohydrates
learn to estimate the number of grams of carbohydrate in the foods you eat
add up the number of grams of carbohydrate from each food you eat to get your total for the day
Your doctor can refer you to a dietitian or diabetes educator who can help you develop a healthy eating plan based on carbohydrate counting.
Which foods contain carbohydrates?
Foods that contain carbohydrates include
grains, such as bread, noodles, pasta, crackers, cereals, and rice
fruits, such as apples, bananas, berries, mangoes, melons, and oranges
dairy products, such as milk and yogurt
legumes, including dried beans, lentils, and peas
snack foods and sweets, such as cakes, cookies, candy, and other desserts
juices, soft drinks, fruit drinks, sports drinks, and energy drinks that contain sugars
vegetables, especially “starchy” vegetables such as potatoes, corn, and peas
Potatoes, peas, and corn are called starchy vegetables because they are high in starch. These vegetables have more carbohydrates per serving than nonstarchy vegetables.
Examples of nonstarchy vegetables are asparagus, broccoli, carrots, celery, green beans, lettuce and other salad greens, peppers, spinach, tomatoes, and zucchini.
Foods that do not contain carbohydrates include meat, fish, and poultry; most types of cheese; nuts; and oils and other fats.
Foods that contain carbohydrates include grains,fruits, dairy products, vegetables, and legumes.
What happens when I eat foods containing carbohydrates?
When you eat foods containing carbohydrates, your digestive system breaks down the sugars and starches into glucose. Glucose is one of the simplest forms of sugar. Glucose then enters your bloodstream from your digestive tract and raises your blood glucose levels. The hormone insulin, which comes from the pancreas or from insulin shots, helps cells throughout your body absorb glucose and use it for energy. Once glucose moves out of the blood into cells, your blood glucose levels go back down.
How can carbohydrate counting help me?
Carbohydrate counting can help keep your blood glucose levels close to normal. Keeping your blood glucose levels as close to normal as possible may help you
stay healthy longer
prevent or delay diabetes problems such as kidney disease, blindness, nerve damage, and blood vessel disease that can lead to heart attacks, strokes, and amputations—surgery to remove a body part
feel better and more energetic
You may also need to take diabetes medicines or have insulin shots to control your blood glucose levels. Discuss your blood glucose targets with your doctor. Targets are numbers you aim for. To meet your targets, you will need to balance your carbohydrate intake with physical activity and diabetes medicines or insulin shots.
How much carbohydrate do I need each day?
The daily amount of carbohydrate, protein, and fat for people with diabetes has not been defined—what is best for one person may not be best for another. Everyone needs to get enough carbohydrate to meet the body’s needs for energy, vitamins and minerals, and fiber.
Experts suggest that carbohydrate intake for most people should be between 45 and 65 percent of total calories. People on low-calorie diets and people who are physically inactive may want to aim for the lower end of that range.
One gram of carbohydrate provides about 4 calories, so you’ll have to divide the number of calories you want to get from carbohydrates by 4 to get the number of grams. For example, if you want to eat 1,800 total calories per day and get 45 percent of your calories from carbohydrates, you would aim for about 200 grams of carbohydrate daily. You would calculate that amount as follows:
.45 x 1,800 calories = 810 calories
810 ÷ 4 = 202.5 grams of carbohydrate
You’ll need to spread out your carbohydrate intake throughout the day. A dietitian or diabetes educator can help you learn what foods to eat, how much to eat, and when to eat based on your weight, activity level, medicines, and blood glucose targets.
How can I find out how much carbohydrate is in the foods I eat?
You will need to learn to estimate the amount of carbohydrate in foods you typically eat. For example, the following amounts of carbohydrate-rich foods each contain about 15 grams of carbohydrate:
one slice of bread
one 6-inch tortilla
1/3 cup of pasta
1/3 cup of rice
1/2 cup of canned or fresh fruit or fruit juice or one small piece of fresh fruit, such as a small apple or orange
1/2 cup of pinto beans
1/2 cup of starchy vegetables such as mashed potatoes, cooked corn, peas, or lima beans
3/4 cup of dry cereal or 1/2 cup cooked cereal
1 tablespoon of jelly
Some foods are so low in carbohydrates that you may not have to count them unless you eat large amounts. For example, most nonstarchy vegetables are low in carbohydrates. A 1/2-cup serving of cooked nonstarchy vegetables or a cup of raw vegetables has only about 5 grams of carbohydrate.
As you become familiar with which foods contain carbohydrates and how many grams of carbohydrate are in food you eat, carbohydrate counting will be easier.
Nutrition Labels
You can find out how many grams of carbohydrate are in the foods you eat by checking the nutrition labels on food packages. Following is an example of a nutrition label:
Nutrition labels tell you the total grams of carbohydrate per serving, along with other nutrition information.
Nutrition labels tell you
the food’s serving size––such as one slice or 1/2 cup
the total grams of carbohydrate per serving
other nutrition information, including calories and the amount of protein and fat per serving
If you have two servings instead of one, such as one cup of pinto beans instead of 1/2 cup, you multiply the number of grams of carbohydrate in one serving—for example, 15—by two to get the total number of grams of carbohydrate—30.
15 x 2 = 30
Cooking at Home
To find out the amount of carbohydrate in homemade foods, you’ll need to estimate and add up the grams of carbohydrate from the ingredients. You can use books or websites that list the typical carbohydrate content of homemade items to estimate the amount of carbohydrate in a serving.
You can also weigh foods with a scale or measure amounts with measuring cups or spoons to estimate the amount of carbohydrate. For example, if a nutrition label shows that 1 1/2 cups of cereal contain 45 grams of carbohydrate, then 1/2 cup will have 15 grams of carbohydrate and 1 cup will have 30 grams of carbohydrate.
Eating Out
Some restaurants provide nutrition information that lists grams of carbohydrate. You can also use carbohydrate counting food lists to estimate the amount of carbohydrate in restaurant meals.
Can I eat sweets and other foods and drinks with added sugars?
Yes, you can eat sweets and other foods and drinks with added sugars. However, you should limit your intake of these high-carbohydrate foods and drinks because they are often high in calories and low in vitamins, minerals, and fiber. Fiber-rich whole grains, fruits, vegetables, and beans are wiser choices.
Instead of eating sweets every day, try eating them in small amounts once in a while so you don’t fill up on foods that are low in nutrition. Ask your dietitian or diabetes educator about including sweets in your eating plan.
How can I tell whether carbohydrate counting is working for me?
Checking your blood glucose levels can help you tell whether carbohydrate counting is working for you. You can check your blood glucose levels using a glucose meter.
You should also have an A1C blood test at least twice a year. The A1C test reflects the average amount of glucose in your blood during the past 3 months.
If your blood glucose levels are too high, you may need to make changes in your eating plan or other lifestyle changes. For example, you may need to make wiser food choices, be more physically active, or make changes to your diabetes medicines. Talk with your doctor about what changes you need to make to control your blood glucose levels.
If you use an insulin pump or take more than one daily insulin shot, ask your doctor how to adjust your insulin when you eat something that isn’t in your usual eating plan.
Can I use carbohydrate counting if I am pregnant?
You can use carbohydrate counting to help control your blood glucose levels when you are pregnant. Meeting your blood glucose targets during pregnancy is important for your and your baby’s health. High blood glucose during pregnancy can harm the baby and increase the baby’s chances of having type 2 diabetes later in life.
Women diagnosed with gestational diabetes—a type of diabetes that develops only during pregnancy—can also use carbohydrate counting to help control their blood glucose levels.
Talk with your doctor about using carbohydrate counting to help meet your blood glucose targets during your pregnancy.
More information about diabetes during pregnancy is provided in the NIDDK health topics:
Where can I find more help with carbohydrate counting?
The Internet has carbohydrate counting tools that let you enter a type of food and find out what nutrients the food contains, including carbohydrates. Try visiting these sites:
Carbohydrate counting is a meal planning tool for people with type 1 or type 2 diabetes. Carbohydrate counting involves keeping track of the amount of carbohydrate in the foods you eat each day.
Carbohydrates are one of the main nutrients found in food and drinks. Carbohydrates include sugars, starches, and fiber.
Carbohydrate counting can help you control your blood glucose, also called blood sugar, levels because carbohydrates affect your blood glucose more than other nutrients.
Carbohydrates are an important part of a healthy eating plan because they provide energy. Most foods containing carbohydrates also contain important vitamins and minerals. Many foods that contain carbohydrates are good sources of fiber, which can help you prevent constipation, lower your cholesterol levels, and control your weight.
To count carbohydrates, you’ll need to know which foods contain carbohydrates and learn to estimate the number of grams of carbohydrate in the foods you eat. Then you’ll add up the number of grams of carbohydrate from each food you eat to get your total for the day.
Foods that contain carbohydrates include grains, fruits, dairy products, vegetables, legumes, snack foods and sweets, and drinks that contain sugar. When you eat carbohydrates, your digestive system breaks down the sugars and starches into glucose.
To meet your blood glucose targets, you will need to balance your carbohydrate intake with physical activity and diabetes medicines or insulin shots.
Nutrition labels on food packages tell you the food’s serving size, the total grams of carbohydrate per serving, and other nutrition information.
Foods and drinks with added sugars are high-carbohydrate foods that are often high in calories and low in vitamins, minerals, and fiber. Fiber-rich whole grains, fruits, vegetables, and beans are wiser choices.
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you? Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open? Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank: Marion J. Franz, M.S., R.D., L.D., C.D.E., Nutrition Concepts by Franz, Inc.; Hope Warshaw, M.M.Sc., R.D., C.D.E., Hope Warshaw Associates, LLC
Fauquier Wellness Center and Inova Diabetes Center Support Group for facilitating field-testing of this publication.
Choose More than 50 Ways to Prevent Type 2 Diabetes
Reduce Portion Sizes
Portion size is the amount of food you eat, such as 1 cup of fruit or 6 ounces of meat. If you are trying to eat smaller portions, eat a half of a bagel instead of a whole bagel or have a 3-ounce hamburger instead of a 6-ounce hamburger. Three ounces is about the size of your fist or a deck of cards.
Put less on your plate, Nate.
1. Drink a large glass of water 10 minutes before your meal so you feel less hungry.
2. Keep meat, chicken, turkey, and fish portions to about 3 ounces.
3. Share one dessert.
Eat a small meal, Lucille.
4. Use teaspoons, salad forks, or child-size forks, spoons, and knives to help you take smaller bites and eat less.
5. Make less food look like more by serving your meal on a salad or breakfast plate.
6. Eat slowly. It takes 20 minutes for your stomach to send a signal to your brain that you are full.
7. Listen to music while you eat instead of watching TV (people tend to eat more while watching TV).
How much should I eat?
Try filling your plate like this:
1/4 protein
1/4 grains
1/2 vegetables and fruit
dairy (low-fat or skim milk)
Move More Each Day
Find ways to be more active each day. Try to be active for at least 30 minutes, 5 days a week. Walking is a great way to get started and you can do it almost anywhere at any time. Bike riding, swimming, and dancing are also good ways to move more.
If you are looking for a safe place to be active, contact your local parks department or health department to ask about walking maps, community centers, and nearby parks.
Dance it away, Faye.
8. Show your kids the dances you used to do when you were their age.
9. Turn up the music and jam while doing household chores.
10. Work out with a video that shows you how to get active.
Let's go, Flo.
11. Deliver a message in person to a co-worker instead of sending an e-mail.
12. Take the stairs to your office. Or take the stairs as far as you can, and then take the elevator the rest of the way.
13. Catch up with friends during a walk instead of by phone.
14. March in place while you watch TV.
15. Choose a place to walk that is safe, such as your local mall.
16. Get off of the bus one stop early and walk the rest of the way home or to work if it is safe.
Make Healthy Food Choices
Find ways to make healthy food choices. This can help you manage your weight and lower your chances of getting type 2 diabetes.
Choose to eat more vegetables, fruits, and whole grains. Cut back on high-fat foods like whole milk, cheeses, and fried foods. This will help you reduce the amount of fat and calories you take in each day.
Snack on a veggie, Reggie.
17. Buy a mix of vegetables when you go food shopping.
18. Choose veggie toppings like spinach, broccoli, and peppers for your pizza.
19. Try eating foods from other countries. Many of these dishes have more vegetables, whole grains, and beans.
20. Buy frozen and low-salt (sodium) canned vegetables. They may cost less and keep longer than fresh ones.
21. Serve your favorite vegetable and a salad with low-fat macaroni and cheese.
Cook with care, Claire.
22. Stir fry, broil, or bake with non-stick spray or low-salt broth. Cook with less oil and butter.
23. Try not to snack while cooking or cleaning the kitchen.
24. Cook with smaller amounts of cured meats (smoked turkey and turkey bacon). They are high in salt.
Cook in style, Kyle.
25. Cook with a mix of spices instead of salt.
26. Try different recipes for baking or broiling meat, chicken, and fish.
27. Choose foods with little or no added sugar to reduce calories.
28. Choose brown rice instead of white rice.
Eat healthy on the go, Jo.
29. Have a big vegetable salad with low-calorie salad dressing when eating out. Share your main dish with a friend or have the other half wrapped to go.
30. Make healthy choices at fast food restaurants. Try grilled chicken (with skin removed) instead of a cheeseburger.
31. Skip the fries and chips and choose a salad.
32. Order a fruit salad instead of ice cream or cake.
Rethink your drink, Linc.
33. Find a water bottle you really like (from a church or club event, favorite sports team, etc.) and drink water from it every day.
34. Peel and eat an orange instead of drinking orange juice.
35. If you drink whole milk, try changing to 2% milk. It has less fat than whole milk. Once you get used to 2% milk, try 1% or fat-free (skim) milk. This will help you reduce the amount of fat and calories you take in each day.
36. Drink water instead of juice and regular soda.
Eat smart, Bart.
37. Make at least half of your grains whole grains, such as whole grain breads and cereals, brown rice, and quinoa.
38. Use whole grain bread for toast and sandwiches.
39. Keep a healthy snack with you, such as fresh fruit, a handful of nuts, and whole grain crackers.
40. Slow down at snack time. Eating a bag of low-fat popcorn takes longer than eating a candy bar.
41. Share a bowl of fruit with family and friends.
42. Eat a healthy snack or meal before shopping for food. Do not shop on an empty stomach.
43. Shop at your local farmers market for fresh, local food.
Keep track, Jack.
44. Make a list of food you need to buy before you go to the store.
45. Keep a written record of what you eat for a week. It can help you see when you tend to overeat or eat foods high in fat or calories.
Read the label, Mabel.
46. Compare food labels on packages.
47. Choose foods lower in saturated fats, trans fats, cholesterol (ko-LESS-tuh-ruhl), calories, salt, and added sugars.
Take Care of Your Mind, Body, and Soul
You can exhale, Gail.
48. Take time to change the way you eat and get active. Try one new food or activity a week.
49. Find ways to relax. Try deep breathing, taking a walk, or listening to your favorite music.
50. Pamper yourself. Read a book, take a long bath, or meditate.
51. Think before you eat. Try not to eat when you are bored, upset, or unhappy.
Be Creative
Honor your health as your most precious gift. There are many more ways to prevent or delay type 2 diabetes by making healthy food choices and moving more. Discover your own and share them with your family, friends, and neighbors.
Make up your own, Tyrone or Simone.
52.
53.
54.
Track Your Progress
Visit National Diabetes Education Program or call 1-888-693-6337 / TTY: 1-866-569-1162 to get your free GAME PLAN to Prevent Type 2 Diabetes booklet. It has charts to help you track the foods you eat and how much you move each day.
Things to Remember:
Talk to your doctor about your risk for getting type 2 diabetes and what you can do to lower your chances.
Take steps to prevent diabetes by making healthy food choices, staying at a healthy weight, and moving more every day.
Find ways to stay calm during your day. Being active and reading a good book can help you lower stress.
Keep track of the many ways you are moving more and eating healthy by writing them down.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Nutrition and physical activity are important parts of a healthy lifestyle when you have diabetes. Along with other benefits, following a healthy meal plan and being active can help you keep your blood glucose level, also called blood sugar, in your target range. To manage your blood glucose, you need to balance what you eat and drink with physical activity and diabetes medicine, if you take any. What you choose to eat, how much you eat, and when you eat are all important in keeping your blood glucose level in the range that your health care team recommends.
Becoming more active and making changes in what you eat and drink can seem challenging at first. You may find it easier to start with small changes and get help from your family, friends, and health care team.
Eating well and being physically active most days of the week can help you
keep your blood glucose level, blood pressure, and cholesterol in your target ranges
You may worry that having diabetes means going without foods you enjoy. The good news is that you can still eat your favorite foods, but you might need to eat smaller portions or enjoy them less often. Your health care team will help create a diabetes meal plan for you that meets your needs and likes.
The key to eating with diabetes is to eat a variety of healthy foods from all food groups, in the amounts your meal plan outlines.
The food groups are
vegetables
nonstarchy: includes broccoli, carrots, greens, peppers, and tomatoes
starchy: includes potatoes, corn, and green peas
fruits—includes oranges, melon, berries, apples, bananas, and grapes
grains—at least half of your grains for the day should be whole grains
includes wheat, rice, oats, cornmeal, barley, and quinoa
examples: bread, pasta, cereal, and tortillas
protein
lean meat
chicken or turkey without the skin
fish
eggs
nuts and peanuts
dried beans and certain peas, such as chickpeas and split peas
beverages with added sugars, such as juice, regular soda, and regular sports or energy drinks
Drink water instead of sweetened beverages. Consider using a sugar substitute in your coffee or tea.
If you drink alcohol, drink moderately—no more than one drink a day if you’re a woman or two drinks a day if you’re a man. If you use insulin or diabetes medicines that increase the amount of insulin your body makes, alcohol can make your blood glucose level drop too low. This is especially true if you haven’t eaten in a while. It’s best to eat some food when you drink alcohol.
When should I eat if I have diabetes?
Some people with diabetes need to eat at about the same time each day. Others can be more flexible with the timing of their meals. Depending on your diabetes medicines or type of insulin, you may need to eat the same amount of carbohydrates at the same time each day. If you take “mealtime” insulin, your eating schedule can be more flexible.
If you use certain diabetes medicines or insulin and you skip or delay a meal, your blood glucose level can drop too low. Ask your health care team when you should eat and whether you should eat before and after physical activity.
How much can I eat if I have diabetes?
Eating the right amount of food will also help you manage your blood glucose level and your weight. Your health care team can help you figure out how much food and how many calories you should eat each day. Look up how many calories are in what you eat and drink at the USDA’s Food-A-Pedia.
Weight-loss planning
If you are overweight or obese, work with your health care team to create a weight-loss plan.
These tools may help:
The Body Weight Planner can help you tailor your plans to reach and maintain your goal weight.
The SuperTracker lets you track your food, physical activity, and weight.
To lose weight, you need to eat fewer calories and replace less healthy foods with foods lower in calories, fat, and sugar.
Two common ways to help you plan how much to eat if you have diabetes are the plate method and carbohydrate counting, also called carb counting. Check with your health care team about the method that’s best for you.
Plate method
The plate method helps you control your portion sizes. You don’t need to count calories. The plate method shows the amount of each food group you should eat. This method works best for lunch and dinner.
Use a 9-inch plate. Put nonstarchy vegetables on half of the plate; a meat or other protein on one-fourth of the plate; and a grain or other starch on the last one-fourth. Starches include starchy vegetables such as corn and peas. You also may eat a small bowl of fruit or a piece of fruit, and drink a small glass of milk as included in your meal plan.
The plate method shows the amount of each food group you should eat.
You can find many different combinations of food and more details about using the plate method from the American Diabetes Association’s Create Your Plate.
Your daily eating plan also may include small snacks between meals.
Portion sizes
You can use everyday objects or your hand to judge the size of a portion.
1 serving of meat or poultry is the palm of your hand or a deck of cards
1 3-ounce serving of fish is a checkbook
1 serving of cheese is six dice
1/2 cup of cooked rice or pasta is a rounded handful or a tennis ball
1 serving of a pancake or waffle is a DVD
2 tablespoons of peanut butter is a ping-pong ball
Carbohydrate counting
Carbohydrate counting involves keeping track of the amount of carbohydrates you eat and drink each day. Because carbohydrates turn into glucose in your body, they affect your blood glucose level more than other foods do. Carb counting can help you manage your blood glucose level. If you take insulin, counting carbohydrates can help you know how much insulin to take.
The right amount of carbohydrates varies by how you manage your diabetes, including how physically active you are and what medicines you take, if any. Your health care team can help you create a personal eating plan based on carbohydrate counting.
The amount of carbohydrates in foods is measured in grams. To count carbohydrate grams in what you eat, you’ll need to
learn which foods have carbohydrates
read the Nutrition Facts food label, or learn to estimate the number of grams of carbohydrate in the foods you eat
add the grams of carbohydrate from each food you eat to get your total for each meal and for the day
Most carbohydrates come from starches, fruits, milk, and sweets. Try to limit carbohydrates with added sugars or those with refined grains, such as white bread and white rice. Instead, eat carbohydrates from fruit, vegetables, whole grains, beans, and low-fat or nonfat milk.
Choose healthy carbohydrates, such as fruit, vegetables, whole grains, beans, and low-fat milk, as part of your diabetes meal plan.
In addition to using the plate method and carb counting, you may want to visit a registered dietitian (RD) for medical nutrition therapy.
What is medical nutrition therapy?
Medical nutrition therapy is a service provided by an RD to create personal eating plans based on your needs and likes. For people with diabetes, medical nutrition therapy has been shown to improve diabetes management. Medicare pays for medical nutrition therapy for people with diabetes. If you have insurance other than Medicare, ask if it covers medical nutrition therapy for diabetes.
Will supplements and vitamins help my diabetes?
No clear proof exists that taking dietary supplements such as vitamins, minerals, herbs, or spices can help manage diabetes.1 You may need supplements if you cannot get enough vitamins and minerals from foods. Talk with your health care provider before you take any dietary supplement since some can cause side effects or affect how your medicines work.2
Why should I be physically active if I have diabetes?
Physical activity is an important part of managing your blood glucose level and staying healthy. Being active has many health benefits.
burns extra calories so you can keep your weight down if needed
improves your mood
can prevent falls and improve memory in older adults
may help you sleep better
If you are overweight, combining physical activity with a reduced-calorie eating plan can lead to even more benefits. In the Look AHEAD: Action for Health in Diabetes study,1 overweight adults with type 2 diabetes who ate less and moved more had greater long-term health benefits compared to those who didn’t make these changes. These benefits included improved cholesterol levels, less sleep apnea, and being able to move around more easily.
Even small amounts of physical activity can help. Experts suggest that you aim for at least 30 minutes of moderate or vigorous physical activity 5 days of the week.3 Moderate activity feels somewhat hard, and vigorous activity is intense and feels hard. If you want to lose weight or maintain weight loss, you may need to do 60 minutes or more of physical activity 5 days of the week.3
Be patient. It may take a few weeks of physical activity before you see changes in your health.
How can I be physically active safely if I have diabetes?
Be sure to drink water before, during, and after exercise to stay well hydrated. The following are some other tips for safe physical activity when you have diabetes.
Drink water when you exercise to stay well hydrated.
Plan ahead
Talk with your health care team before you start a new physical activity routine, especially if you have other health problems. Your health care team will tell you a target range for your blood glucose level and suggest how you can be active safely.
Your health care team also can help you decide the best time of day for you to do physical activity based on your daily schedule, meal plan, and diabetes medicines. If you take insulin, you need to balance the activity that you do with your insulin doses and meals so you don’t get low blood glucose.
Prevent low blood glucose
Because physical activity lowers your blood glucose, you should protect yourself against low blood glucose levels, also called hypoglycemia. You are most likely to have hypoglycemia if you take insulin or certain other diabetes medicines, such as a sulfonylurea. Hypoglycemia also can occur after a long intense workout or if you have skipped a meal before being active. Hypoglycemia can happen during or up to 24 hours after physical activity.
Planning is key to preventing hypoglycemia. For instance, if you take insulin, your health care provider might suggest you take less insulin or eat a small snack with carbohydrates before, during, or after physical activity, especially intense activity.4
You may need to check your blood glucose level before, during, and right after you are physically active.
Take care of your feet
People with diabetes may have problems with their feet because of poor blood flow and nerve damage that can result from high blood glucose levels. To help prevent foot problems, you should wear comfortable, supportive shoes and take care of your feet before, during, and after physical activity.
What physical activities should I do if I have diabetes?
Most kinds of physical activity can help you take care of your diabetes. Certain activities may be unsafe for some people, such as those with low vision or nerve damage to their feet. Ask your health care team what physical activities are safe for you. Many people choose walking with friends or family members for their activity.
Doing different types of physical activity each week will give you the most health benefits. Mixing it up also helps reduce boredom and lower your chance of getting hurt. Try these options for physical activity.
Add extra activity to your daily routine
If you have been inactive or you are trying a new activity, start slowly, with 5 to 10 minutes a day. Then add a little more time each week. Increase daily activity by spending less time in front of a TV or other screen. Try these simple ways to add physical activities in your life each day:
Walk around while you talk on the phone or during TV commercials.
Do chores, such as work in the garden, rake leaves, clean the house, or wash the car.
Park at the far end of the shopping center parking lot and walk to the store.
Take the stairs instead of the elevator.
Make your family outings active, such as a family bike ride or a walk in a park.
If you are sitting for a long time, such as working at a desk or watching TV, do some light activity for 3 minutes or more every half hour.5 Light activities include
leg lifts or extensions
overhead arm stretches
desk chair swivels
torso twists
side lunges
walking in place
Do aerobic exercise
Aerobic exercise is activity that makes your heart beat faster and makes you breathe harder. You should aim for doing aerobic exercise for 30 minutes a day most days of the week. You do not have to do all the activity at one time. You can split up these minutes into a few times throughout the day.
To get the most out of your activity, exercise at a moderate to vigorous level. Try
walking briskly or hiking
climbing stairs
swimming or a water-aerobics class
dancing
riding a bicycle or a stationary bicycle
taking an exercise class
playing basketball, tennis, or other sports
Talk with your health care team about how to warm up and cool down before and after you exercise.
Do strength training to build muscle
Strength training is a light or moderate physical activity that builds muscle and helps keep your bones healthy. Strength training is important for both men and women. When you have more muscle and less body fat, you’ll burn more calories. Burning more calories can help you lose and keep off extra weight.
You can do strength training with hand weights, elastic bands, or weight machines. Try to do strength training two to three times a week. Start with a light weight. Slowly increase the size of your weights as your muscles become stronger.
You can do strength training with hand weights, elastic bands, or weight machines.
Do stretching exercises
Stretching exercises are light or moderate physical activity. When you stretch, you increase your flexibility, lower your stress, and help prevent sore muscles.
You can choose from many types of stretching exercises. Yoga is a type of stretching that focuses on your breathing and helps you relax. Even if you have problems moving or balancing, certain types of yoga can help. For instance, chair yoga has stretches you can do when sitting in a chair or holding onto a chair while standing. Your health care team can suggest whether yoga is right for you.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Your health care professional can diagnose diabetes, prediabetes, and gestational diabetes through blood tests. The blood tests show if your blood glucose, also called blood sugar, is too high.
Do not try to diagnose yourself if you think you might have diabetes. Testing equipment that you can buy over the counter, such as a blood glucose meter, cannot diagnose diabetes.
Who should be tested for diabetes?
Anyone who has symptoms of diabetes should be tested for the disease. Some people will not have any symptoms but may have risk factors for diabetes and need to be tested. Testing allows health care professionals to find diabetes sooner and work with their patients to manage diabetes and prevent complications.
Testing also allows health care professionals to find prediabetes. Making lifestyle changes to lose a modest amount of weight if you are overweight may help you delay or prevent type 2 diabetes.
Blood tests help health care professionals diagnose diabetes and prediabetes.
Type 1 diabetes
Most often, testing for occurs in people with diabetes symptoms. Doctors usually diagnose type 1 diabetes in children and young adults. Because type 1 diabetes can run in families, a study called TrialNet offers free testing to family members of people with the disease, even if they don’t have symptoms.
Type 2 diabetes
Experts recommend routine testing for type 2 diabetes if you
are age 45 or older
are between the ages of 19 and 44, are overweight or obese, and have one or more other diabetes risk factors
are a woman who had gestational diabetes1
Medicare covers the cost of diabetes tests for people with certain risk factors for diabetes. If you have Medicare, find out if you qualify for coverage. If you have different insurance, ask your insurance company if it covers diabetes tests.
Though type 2 diabetes most often develops in adults, children also can develop type 2 diabetes. Experts recommend testing children between the ages of 10 and 18 who are overweight or obese and have at least two other risk factors for developing diabetes.1
low birthweight
a mother who had diabetes while pregnant with them
All pregnant women who do not have a prior diabetes diagnosis should be tested for gestational diabetes. If you are pregnant, you will take a glucose challenge test between 24 and 28 weeks of pregnancy.1
What tests are used to diagnose diabetes and prediabetes?
Health care professionals most often use the fasting plasma glucose (FPG) test or the A1C test to diagnose diabetes. In some cases, they may use a random plasma glucose (RPG) test.
Fasting plasma glucose (FPG) test
The FPG blood test measures your blood glucose level at a single point in time. For the most reliable results, it is best to have this test in the morning, after you fast for at least 8 hours. Fasting means having nothing to eat or drink except sips of water.
A1C test
The A1C test is a blood test that provides your average levels of blood glucose over the past 3 months. Other names for the A1C test are hemoglobin A1C, HbA1C, glycated hemoglobin, and glycosylated hemoglobin test. You can eat and drink before this test. When it comes to using the A1C to diagnose diabetes, your doctor will consider factors such as your age and whether you have anemia or another problem with your blood.1 The A1C test is not accurate in people with anemia.
Your health care professional will report your A1C test result as a percentage, such as an A1C of 7 percent. The higher the percentage, the higher your average blood glucose levels.
People with diabetes also use information from the A1C test to help manage their diabetes.
Random plasma glucose (RPG) test
Sometimes health care professionals use the RPG test to diagnose diabetes when diabetes symptoms are present and they do not want to wait until you have fasted. You do not need to fast overnight for the RPG test. You may have this blood test at any time.
What tests are used to diagnose gestational diabetes?
Pregnant women may have the glucose challenge test, the oral glucose tolerance test, or both. These tests show how well your body handles glucose.
Glucose challenge test
If you are pregnant and a health care professional is checking you for gestational diabetes, you may first receive the glucose challenge test. Another name for this test is the glucose screening test. In this test, a health care professional will draw your blood 1 hour after you drink a sweet liquid containing glucose. You do not need to fast for this test. If your blood glucose is too high—135 to 140 or more—you may need to return for an oral glucose tolerance test while fasting.
Oral glucose tolerance test (OGTT)
The OGTT measures blood glucose after you fast for at least 8 hours. First, a health care professional will draw your blood. Then you will drink the liquid containing glucose. For diagnosing gestational diabetes, you will need your blood drawn every hour for 2 to 3 hours.
High blood glucose levels at any two or more blood test times during the OGTT—fasting, 1 hour, 2 hours, or 3 hours—mean you have gestational diabetes. Your health care team will explain what your OGTT results mean.
Health care professionals also can use the OGTT to diagnose type 2 diabetes and prediabetes in people who are not pregnant. The OGTT helps health care professionals detect type 2 diabetes and prediabetes better than the FPG test. However, the OGTT is a more expensive test and is not as easy to give. To diagnose type 2 diabetes and prediabetes, a health care professional will need to draw your blood 1 hour after you drink the liquid containing glucose and again after 2 hours.
What test numbers tell me if I have diabetes or prediabetes?
Each test to detect diabetes and prediabetes uses a different measurement. Usually, the same test method needs to be repeated on a second day to diagnose diabetes. Your doctor may also use a second test method to confirm that you have diabetes.
The following table helps you understand what your test numbers mean if you are not pregnant.
Diagnosis
A1C (percent)
Fasting plasma glucose (FPG)a
Oral glucose tolerance test (OGTT)ab
Random plasma glucose test (RPG)a
Normal
below 5.7
99 or below
139 or below
Prediabetes
5.7 to 6.4
100 to 125
140 to 199
Diabetes
6.5 or above
126 or above
200 or above
200 or above
Which tests help my health care professional know what kind of diabetes I have?
Even though the tests described here can confirm that you have diabetes, they can’t identify what type you have. Sometimes health care professionals are unsure if diabetes is type 1 or type 2. A rare type of diabetes that can occur in babies, called monogenic diabetes, can also be mistaken for type 1 diabetes. Treatment depends on the type of diabetes, so knowing which type you have is important.
To find out if your diabetes is type 1, your health care professional may look for certain autoantibodies. Autoantibodies are antibodies that mistakenly attack your healthy tissues and cells. The presence of one or more of several types of autoantibodies specific to diabetes is common in type 1 diabetes, but not in type 2 or monogenic diabetes. A health care professional will have to draw your blood for this test.
If you had diabetes while you were pregnant, you should get tested 6 to 12 weeks after your baby is born to see if you have type 2 diabetes.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Foot problems are common in people with diabetes. You might be afraid you’ll lose a toe, foot, or leg to diabetes, or know someone who has, but you can lower your chances of having diabetes-related foot problems by taking care of your feet every day. Managing your blood glucose levels, also called blood sugar, can also help keep your feet healthy.
How can diabetes affect my feet?
Over time, diabetes may cause nerve damage, also called diabetic neuropathy, that can cause tingling and pain, and can make you lose feeling in your feet. When you lose feeling in your feet, you may not feel a pebble inside your sock or a blister on your foot, which can lead to cuts and sores. Cuts and sores can become infected.
Diabetes also can lower the amount of blood flow in your feet. Not having enough blood flowing to your legs and feet can make it hard for a sore or an infection to heal. Sometimes, a bad infection never heals. The infection might lead to gangrene.
Gangrene and foot ulcers that do not get better with treatment can lead to an amputation of your toe, foot, or part of your leg. A surgeon may perform an amputation to prevent a bad infection from spreading to the rest of your body, and to save your life. Good foot care is very important to prevent serious infections and gangrene.
Although rare, nerve damage from diabetes can lead to changes in the shape of your feet, such as Charcot’s foot. Charcot’s foot may start with redness, warmth, and swelling. Later, bones in your feet and toes can shift or break, which can cause your feet to have an odd shape, such as a “rocker bottom.”
Charcot’s foot can cause your feet to have an odd shape, such as a “rocker bottom.”
What can I do to keep my feet healthy?
Work with your health care team to make a diabetes self-care plan, which is an action plan for how you will manage your diabetes. Your plan should include foot care. A foot doctor, also called a podiatrist, and other specialists may be part of your health care team.
Include these steps in your foot care plan:
Check your feet every day
You may have foot problems, but feel no pain in your feet. Checking your feet each day will help you spot problems early before they get worse. A good way to remember is to check your feet each evening when you take off your shoes. Also check between your toes. If you have trouble bending over to see your feet, try using a mirror to see them, or ask someone else to look at your feet.
Look for problems such as
cuts, sores, or red spots
swelling or fluid-filled blisters
ingrown toenails, in which the edge of your nail grows into your skin
corns or calluses, which are spots of rough skin caused by too much rubbing or pressure on the same spot
plantar warts, which are flesh-colored growths on the bottom of the feet
If you have certain foot problems that make it more likely you will develop a sore on your foot, your doctor may recommend taking the temperature of the skin on different parts of your feet. A “hot spot” can be the first sign that a blister or an ulcer is starting.
Cover a blister, cut, or sore with a bandage. Smooth corns and calluses as explained below.
Wash your feet every day
Wash your feet with soap in warm, not hot, water. Test the water to make sure it is not too hot. You can use a thermometer (90° to 95° F is safe) or your elbow to test the warmth of the water. Do not soak your feet because your skin will get too dry.
After washing and drying your feet, put talcum powder or cornstarch between your toes. Skin between the toes tends to stay moist. Powder will keep the skin dry to help prevent an infection.
Smooth corns and calluses gently
Thick patches of skin called corns or calluses can grow on the feet. If you have corns or calluses, talk with your foot doctor about the best way to care for these foot problems. If you have nerve damage, these patches can become ulcers.
If your doctor tells you to, use a pumice stone to smooth corns and calluses after bathing or showering. A pumice stone is a type of rock used to smooth the skin. Rub gently, only in one direction, to avoid tearing the skin.
Do NOT
cut corns and calluses
use corn plasters, which are medicated pads
use liquid corn and callus removers
Cutting and over-the counter corn removal products can damage your skin and cause an infection.
To keep your skin smooth and soft, rub a thin coat of lotion, cream, or petroleum jelly on the tops and bottoms of your feet. Do not put lotion or cream between your toes because moistness might cause an infection.
Trim your toenails straight across
Trim your toenails, when needed, after you wash and dry your feet. Using toenail clippers, trim your toenails straight across. Do not cut into the corners of your toenail. Gently smooth each nail with an emery board or nonsharp nail file. Trimming this way helps prevent cutting your skin and keeps the nails from growing into your skin.
Have a foot doctor trim your toenails if
you cannot see, feel, or reach your feet
your toenails are thick or yellowed
your nails curve and grow into the skin
If you want to get a pedicure at a salon, you should bring your own nail tools to prevent getting an infection. You can ask your health care provider what other steps you can take at the salon to prevent infection.
Wear shoes and socks at all times
Wear shoes and socks at all times. Do not walk barefoot or in just socks – even when you are indoors. You could step on something and hurt your feet. You may not feel any pain and may not know that you hurt yourself.
Check the inside of your shoes before putting them on, to make sure the lining is smooth and free of pebbles or other objects.
Make sure you wear socks, stockings, or nylons with your shoes to keep from getting blisters and sores. Choose clean, lightly padded socks that fit well. Socks with no seams are best.
Wear shoes that fit well and protect your feet. Here are some tips for finding the right type of shoes:
Walking shoes and athletic shoes are good for daily wear. They support your feet and allow them to “breathe.”
Do not wear vinyl or plastic shoes, because they do not stretch or “breathe.”
When buying shoes, make sure they feel good and have enough room for your toes. Buy shoes at the end of the day, when your feet are the largest, so that you can find the best fit.
If you have a bunion, or hammertoes, which are toes that curl under your feet, you may need extra-wide or deep shoes.1 Do not wear shoes with pointed toes or high heels, because they put too much pressure on your toes.
If your feet have changed shape, such as from Charcot’s foot, you may need special shoes or shoe inserts, called orthotics. You also may need inserts if you have bunions, hammertoes, or other foot problems.
When breaking in new shoes, only wear them for a few hours at first and then check your feet for areas of soreness.
Medicare Part B insurance and other health insurance programs may help pay for these special shoes or inserts. Ask your insurance plan if it covers your special shoes or inserts.
Protect your feet from hot and cold
If you have nerve damage from diabetes, you may burn your feet and not know you did. Take the following steps to protect your feet from heat:
Wear shoes at the beach and on hot pavement.
Put sunscreen on the tops of your feet to prevent sunburn.
Keep your feet away from heaters and open fires.
Do not put a hot water bottle or heating pad on your feet.
Wear socks in bed if your feet get cold. In the winter, wear lined, waterproof boots to keep your feet warm and dry.
Keep the blood flowing to your feet
Try the following tips to improve blood flow to your feet:
Put your feet up when you are sitting.
Wiggle your toes for a few minutes throughout the day. Move your ankles up and down and in and out to help blood flow in your feet and legs.
Do not wear tight socks or elastic stockings. Do not try to hold up loose socks with rubber bands.
Be more physically active. Choose activities that are easy on your feet, such as walking, dancing, yoga or stretching, swimming, or bike riding.
Stop smoking.
Smoking can lower the amount of blood flow to your feet. If you smoke, ask for help to stop. You can get help by calling the national quitline at 1-800-QUITNOW or 1-800-784-8669. For tips on quitting, go to SmokeFree.gov.
Get a foot check at every health care visit
Ask your health care team to check your feet at each visit. Take off your shoes and socks when you’re in the exam room so they will remember to check your feet. At least once a year, get a thorough foot exam, including a check of the feeling and pulses in your feet.
Get a thorough foot exam at each health care visit if you have
Ask your health care team to show you how to care for your feet.
When should I see my health care provider about foot problems?
Call your health care provider right away if you have
a cut, blister, or bruise on your foot that does not start to heal after a few days
skin on your foot that becomes red, warm, or painful—signs of a possible infection
a callus with dried blood inside of it,which often can be the first sign of a wound under the callus
a foot infection that becomes black and smelly—signs you might have gangrene
Ask your provider to refer you to a foot doctor, or podiatrist, if needed.
References
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
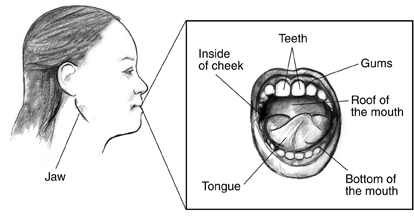
Too much glucose, also called sugar, in your blood from diabetes can cause pain, infection, and other problems in your mouth. Your mouth includes
your teeth
your gums
your jaw
tissues such as your tongue, the roof and bottom of your mouth, and the inside of your cheeks
Glucose is present in your saliva—the fluid in your mouth that makes it wet. When diabetes is not controlled, high glucose levels in your saliva help harmful bacteria grow. These bacteria combine with food to form a soft, sticky film called plaque. Plaque also comes from eating foods that contain sugars or starches. Some types of plaque cause tooth decay or cavities. Other types of plaque cause gum disease and bad breath.
Gum disease can be more severe and take longer to heal if you have diabetes. In turn, having gum disease can make your blood glucose hard to control.
What happens if I have plaque?
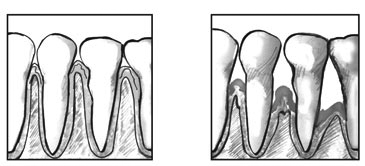
Plaque that is not removed hardens over time into tartar and collects above your gum line. Tartar makes it more difficult to brush and clean between your teeth. Your gums become red and swollen, and bleed easily—signs of unhealthy or inflamed gums, called gingivitis.
When gingivitis is not treated, it can advance to gum disease called periodontitis. In periodontitis, the gums pull away from the teeth and form spaces, called pockets, which slowly become infected. This infection can last a long time. Your body fights the bacteria as the plaque spreads and grows below the gum line. Both the bacteria and your body’s response to this infection start to break down the bone and the tissue that hold the teeth in place. If periodontitis is not treated, the gums, bones, and tissue that support the teeth are destroyed. Teeth may become loose and might need to be removed. If you have periodontitis, your dentist may send you to a periodontist, an expert in treating gum disease.
Healthy gums
Periodontitis
What are the most common mouth problems from diabetes?
The following chart shows the most common mouth problems from diabetes.
Problem
What It Is
Symptoms
Treatment
gingivitis
unhealthy or inflamed gums
red, swollen, and bleeding gums
daily brushing and flossing
regular cleanings at the dentist
periodontitis
gum disease, which can change from mild to severe
red, swollen, and bleeding gums
gums that have pulled away from the teeth
long-lasting infection between the teeth and gums
bad breath that won’t go away
permanent teeth that are loose or moving away from one another
changes in the way your teeth fit together when you bite
sometimes pus between the teeth and gums
changes in the fit of dentures, which are teeth you can remove
deep cleaning at your dentist
medicine that your dentist prescribes
gum surgery in severe cases
thrush, called candidiasis
the growth of a naturally occurring fungus that the body is unable to control
sore, white—or sometimes red—patches on your gums, tongue, cheeks, or the roof of your mouth
patches that have turned into open sores
medicine that your doctor or dentist prescribes to kill the fungus
cleaning dentures
removing dentures for part of the day or night, and soaking them in medicine that your doctor or dentist prescribes
dry mouth, called xerostomia
a lack of saliva in your mouth, which raises your risk for tooth decay and gum disease
dry feeling in your mouth, often or all of the time
dry, rough tongue
pain in the mouth
cracked lips
mouth sores or infection
problems chewing, eating, swallowing, or talking
taking medicine to keep your mouth wet that your doctor or dentist prescribes
rinsing with a fluoride mouth rinse to prevent cavities
using sugarless gum or mints to increase saliva flow
taking frequent sips of water
avoiding tobacco, caffeine, and alcoholic beverages
using a humidifier, a device that raises the level of moisture in your home, at night
avoiding spicy or salty foods that may cause pain in a dry mouth
oral burning
a burning sensation inside the mouth caused by uncontrolled blood glucose levels
burning feeling in the mouth
dry mouth
bitter taste
symptoms may worsen throughout the day
seeing your doctor, who may change your diabetes medicine
once your blood glucose is under control, the oral burning will go away
More symptoms of a problem in your mouth are
a sore, or an ulcer, that does not heal
dark spots or holes in your teeth
pain in your mouth, face, or jaw that doesn’t go away
loose teeth
pain when chewing
a changed sense of taste or a bad taste in your mouth
bad breath that doesn’t go away when you brush your teeth
How will I know if I have mouth problems from diabetes?
Check your mouth for signs of problems from diabetes. If you notice any problems, see your dentist right away. Some of the first signs of gum disease are swollen, tender, or bleeding gums. Sometimes you won’t have any signs of gum disease. You may not know you have it until you have serious damage. Your best defense is to see your dentist twice a year for a cleaning and checkup.
Check your mouth for signs of problems from diabetes.
How can I prepare for a visit to my dentist?
Plan ahead. Talk with your doctor and dentist before the visit about the best way to take care of your blood glucose during dental work.
You may be taking a diabetes medicine that can cause low blood glucose, also called hypoglycemia. If you take insulin or other diabetes medicines, take them and eat as usual before visiting the dentist. You may need to bring your diabetes medicines and your snacks or meal with you to the dentist’s office.
You may need to postpone any nonemergency dental work if your blood glucose is not under control.
If you feel nervous about visiting the dentist, tell your dentist and the staff about your feelings. Your dentist can adapt the treatment to your needs. Don’t let your nerves stop you from having regular checkups. Waiting too long to take care of your mouth may make things worse.
If you feel nervous about visiting the dentist, tell your dentist and the staff about your feelings.
If you feel nervous about visiting the dentist, tell your dentist and the staff about your feelings.
What if my mouth is sore after my dental work?
A sore mouth is common after dental work. If this happens, you might not be able to eat or chew the foods you normally eat for several hours or days. For guidance on how to adjust your usual routine while your mouth is healing, ask your doctor
what foods and drinks you should have
if you should change the time when you take your diabetes medicines
if you should change the dose of your diabetes medicines
how often you should check your blood glucose
How does smoking affect my mouth?
Smoking makes problems with your mouth worse. Smoking raises your chances of getting gum disease, oral and throat cancers, and oral fungal infections. Smoking also discolors your teeth and makes your breath smell bad.
Smoking and diabetes are a dangerous mix. Smoking raises your risk for many diabetes problems. If you quit smoking,
you will lower your risk for heart attack, stroke, nerve disease, kidney disease, and amputation
your cholesterol and blood pressure levels might improve
your blood circulation will improve
If you smoke, stop smoking. Ask for help so that you don’t have to do it alone. You can start by calling 1–800–QUITNOW or 1–800–784–8669.
How can I keep my mouth healthy?
You can keep your mouth healthy by taking these steps:
Keep your blood glucose numbers as close to your target as possible. Your doctor will help you set your target blood glucose numbers and teach you what to do if your numbers are too high or too low.
Eat healthy meals and follow the meal plan that you and your doctor or dietitian have worked out.
Brush your teeth at least twice a day with fluoride toothpaste. Fluoride protects against tooth decay.
Aim for brushing first thing in the morning, before going to bed, and after each meal and sugary or starchy snack.
Use a soft toothbrush.
Gently brush your teeth with the toothbrush angled towards the gum line.
Use small, circular motions.
Brush the front, back, and top of each tooth. Brush your tongue, too.
Change your toothbrush every 3 months or sooner if the toothbrush looks worn or the bristles spread out. A new toothbrush removes more plaque.
Drink water that contains added fluoride or ask your dentist about using a fluoride mouth rinse to prevent tooth decay.
Ask your dentist about using an anti-plaque or anti-gingivitis mouth rinse to control plaque or prevent gum disease.
Use dental floss to clean between your teeth at least once a day. Flossing helps prevent plaque from building up on your teeth. When flossing,
slide the floss up and down and then curve it around the base of each tooth under the gums
use clean sections of floss as you move from tooth to tooth
Another way of removing plaque between teeth is to use a dental pick or brush—thin tools designed to clean between the teeth. You can buy these picks at drug stores or grocery stores.
If you wear dentures, keep them clean and take them out at night. Have them adjusted if they become loose or uncomfortable.
Call your dentist right away if you have any symptoms of mouth problems.
See your dentist twice a year for a cleaning and checkup. Your dentist may suggest more visits if you need them.
See your dentist twice a year for a cleaning and checkup.
Follow your dentist’s advice.
If your dentist tells you about a problem, take care of it right away.
Follow any steps or treatments from your dentist to keep your mouth healthy.
Tell your dentist that you have diabetes.
Tell your dentist about any changes in your health or medicines.
Share the results of some of your diabetes blood tests, such as the A1C test or the fasting blood glucose test.
Ask if you need antibiotics before and after dental treatment if your diabetes is uncontrolled.
If you smoke, stop smoking.
This information may contain content about medications and, when taken as prescribed, the conditions they treat. When prepared, this content included the most current information available. For updates or for questions about any medications, contact the U.S. Food and Drug Administration toll-free at 1-888-INFO-FDA (1-888-463-6332) or visit
www.fda.gov. Consult your health care provider for more information.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Having diabetes means that you are more likely to develop heart disease and have a greater chance of a heart attack or a stroke. People with diabetes are also more likely to have certain conditions, or risk factors, that increase the chances of having heart disease or stroke, such as high blood pressure or high cholesterol. If you have diabetes, you can protect your heart and health by managing your blood glucose, also called blood sugar, as well as your blood pressure and cholesterol. If you smoke, get help to stop.
What is the link between diabetes, heart disease, and stroke?
Over time, high blood glucose from diabetes can damage your blood vessels and the nerves that control your heart and blood vessels. The longer you have diabetes, the higher the chances that you will develop heart disease.1
People with diabetes tend to develop heart disease at a younger age than people without diabetes. In adults with diabetes, the most common causes of death are heart disease and stroke. Adults with diabetes are nearly twice as likely to die from heart disease or stroke as people without diabetes.2
What else increases my chances of heart disease or stroke if I have diabetes?
If you have diabetes, other factors add to your chances of developing heart disease or having a stroke.
Smoking
Smoking raises your risk of developing heart disease. If you have diabetes, it is important to stop smoking because both smoking and diabetes narrow blood vessels. Smoking also increases your chances of developing other long-term problems such as lung disease. Smoking also can damage the blood vessels in your legs and increase the risk of lower leg infections, ulcers, and amputation.
High blood pressure
If you have high blood pressure, your heart must work harder to pump blood. High blood pressure can strain your heart, damage blood vessels, and increase your risk of heart attack, stroke, eye problems, and kidney problems.
Abnormal cholesterol levels
Cholesterol is a type of fat produced by your liver and found in your blood. You have two kinds of cholesterol in your blood: LDL and HDL.
LDL, often called “bad” cholesterol, can build up and clog your blood vessels. High levels of LDL cholesterol raise your risk of developing heart disease.
Another type of blood fat, triglycerides, also can raise your risk of heart disease when the levels are higher than recommended by your health care team.
Obesity and belly fat
Being overweight or obese can affect your ability to manage your diabetes and increase your risk for many health problems, including heart disease and high blood pressure. If you are overweight, a healthy eating plan with reduced calories often will lower your glucose levels and reduce your need for medications.
Excess belly fat around your waist, even if you are not overweight, can raise your chances of developing heart disease.
Even if you are a normal weight, excess belly fat can raise your risk for heart disease.
A family history of heart disease may also add to your chances of developing heart disease. If one or more of your family members had a heart attack before age 50, you may have an even higher chance of developing heart disease.3
You can’t change whether heart disease runs in your family, but if you have diabetes, it’s even more important to take steps to protect yourself from heart disease and decrease your chances of having a stroke.
How can I lower my chances of a heart attack or stroke if I have diabetes?
Taking care of your diabetes is important to help you take care of your heart. You can lower your chances of having a heart attack or stroke by taking the following steps to manage your diabetes to keep your heart and blood vessels healthy.
Manage your diabetes ABCs
Knowing your diabetes ABCs will help you manage your blood glucose, blood pressure, and cholesterol. Stopping smoking if you have diabetes is also important to lower your chances for heart disease.
A is for the A1C test. The A1C test shows your average blood glucose level over the past 3 months. This is different from the blood glucose checks that you do every day. The higher your A1C number, the higher your blood glucose levels have been during the past 3 months. High levels of blood glucose can harm your heart, blood vessels, kidneys, feet, and eyes.
The A1C goal for many people with diabetes is below 7 percent. Some people may do better with a slightly higher A1C goal. Ask your health care team what your goal should be.
B is for blood pressure. Blood pressure is the force of your blood against the wall of your blood vessels. If your blood pressure gets too high, it makes your heart work too hard. High blood pressure can cause a heart attack or stroke and damage your kidneys and eyes.
The blood pressure goal for most people with diabetes is below 140/90 mm Hg. Ask what your goal should be.
C is for cholesterol. You have two kinds of cholesterol in your blood: LDL and HDL. LDL or “bad” cholesterol can build up and clog your blood vessels. Too much bad cholesterol can cause a heart attack or stroke. HDL or “good” cholesterol helps remove the “bad” cholesterol from your blood vessels.
Ask your health care team what your cholesterol numbers should be. If you are over 40 years of age, you may need to take medicine such as a statin to lower your cholesterol and protect your heart. Some people with very high LDL (“bad”) cholesterol may need to take medicine at a younger age.
S is for stop smoking. Not smoking is especially important for people with diabetes because both smoking and diabetes narrow blood vessels, so your heart has to work harder.
If you quit smoking
you will lower your risk for heart attack, stroke, nerve disease, kidney disease, eye disease, and amputation
your blood glucose, blood pressure, and cholesterol levels may improve
your blood circulation will improve
you may have an easier time being physically active
If you smoke or use other tobacco products, stop. Ask for help so you don’t have to do it alone. You can start by calling the national quitline at 1-800-QUITNOW or 1-800-784-8669. For tips on quitting, go to Smokefree.gov.
Ask your health care team about your goals for A1C, blood pressure, and cholesterol, and what you can do to reach these goals.
Managing diabetes is not always easy. Feeling stressed, sad, or angry is common when you are living with diabetes. You may know what to do to stay healthy but may have trouble sticking with your plan over time. Long-term stress can raise your blood glucose and blood pressure, but you can learn ways to lower your stress. Try deep breathing, gardening, taking a walk, doing yoga, meditating, doing a hobby, or listening to your favorite music. Learn more about healthy ways to cope with stress.
Take medicine to protect your heart
Medicines may be an important part of your treatment plan. Your doctor will prescribe medicine based on your specific needs. Medicine may help you
meet your A1C (blood glucose), blood pressure, and cholesterol goals.
reduce your risk of blood clots, heart attack, or stroke.
treat angina, or chest pain that is often a symptom of heart disease. (Angina can also be an early symptom of a heart attack.)
Ask your doctor whether you should take aspirin. Aspirin is not safe for everyone. Your doctor can tell you whether taking aspirin is right for you and exactly how much to take.
Statins can reduce the risk of having a heart attack or stroke in some people with diabetes. Statins are a type of medicine often used to help people meet their cholesterol goals. Talk with your doctor to find out whether taking a statin is right for you.
Talk with your doctor if you have questions about your medicines. Before you start a new medicine, ask your doctor about possible side effects and how you can avoid them. If the side effects of your medicine bother you, tell your doctor. Don’t stop taking your medicines without checking with your doctor first.
Take medicines as prescribed.
How do doctors diagnose heart disease in diabetes?
Tests used to monitor your diabetes—A1C, blood pressure, and cholesterol—help your doctor decide whether it is important to do other tests to check your heart health.
Your health care provider will do a physical exam.
What are the warning signs of heart attack and stroke?
Call 9-1-1 right away if you have warning signs of a heart attack:
pain or pressure in your chest that lasts longer than a few minutes or goes away and comes back
pain or discomfort in one or both of your arms or shoulders; or your back, neck, or jaw
shortness of breath
sweating or light-headedness
indigestion or nausea (feeling sick to your stomach)
feeling very tired
Treatment works best when it is given right away. Warning signs can be different in different people. You may not have all of these symptoms.
Call 9-1-1 right away if you have warning signs of a stroke, including sudden
weakness or numbness of your face, arm, or leg on one side of your body
confusion, or trouble talking or understanding
dizziness, loss of balance, or trouble walking
trouble seeing out of one or both eyes
sudden severe headache
If you have any one of these warning signs, call 9-1-1. You can help prevent permanent damage by getting to a hospital within an hour of a stroke.
Call 9-1-1 if you have the warning signs of a heart attack or stroke. Treatment works best when given right away.
References
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
John B. Buse, M.D., Ph.D., Chief, Division of Endocrinology; Director, NC Translational and Clinical Sciences Institute; University of North Carolina School of Medicine
Diabetes is the leading cause of kidney disease. About 1 out of 4 adults with diabetes has kidney disease.1
The main job of the kidneys is to filter wastes and extra water out of your blood to make urine. Your kidneys also help control blood pressure and make hormones that your body needs to stay healthy.
Your kidneys are located in the middle of your back, just below your rib cage.
When your kidneys are damaged, they can’t filter blood like they should, which can cause wastes to build up in your body. Kidney damage can also cause other health problems.
Kidney damage caused by diabetes usually occurs slowly, over many years. You can take steps to protect your kidneys and to prevent or delay kidney damage.
What increases my chances of developing diabetic kidney disease?
Having diabetes for a longer time increases the chances that you will have kidney damage. If you have diabetes, you are more likely to develop kidney disease if your
blood glucose is too high
blood pressure is too high
African Americans, American Indians, and Hispanics/Latinos develop diabetes, kidney disease, and kidney failure at a higher rate than Caucasians.
You are also more likely to develop kidney disease if you have diabetes and
If you have diabetes, you are more likely to develop kidney disease if you have high blood pressure.
How can I tell if I have diabetic kidney disease?
Most people with diabetic kidney disease do not have symptoms. The only way to know if you have diabetic kidney disease is to get your kidneys checked.
Health care professionals use blood and urine tests to check for diabetic kidney disease. Your health care professional will check your urine for albumin and will also do a blood test to see how well your kidneys are filtering your blood.
You should get tested every year for kidney disease if you
Health care professionals use blood and urine tests to check for kidney disease.
How can I keep my kidneys healthy if I have diabetes?
The best way to slow or prevent diabetes-related kidney disease is to try to reach your blood glucose and blood pressure goals. Healthy lifestyle habits and taking your medicines as prescribed can help you achieve these goals and improve your health overall.
Reach your blood glucose goals
Your health care professional will test your A1C. The A1C is a blood test that shows your average blood glucose level over the past 3 months. This is different from the blood glucose checks that you may do yourself. The higher your A1C number, the higher your blood glucose levels have been during the past 3 months.
The A1C goal for many people with diabetes is below 7 percent. Ask your health care team what your goal should be. Reaching your goal numbers will help you protect your kidneys.
To reach your A1C goal, your health care professional may ask you to check your blood glucose levels. Work with your health care team to use the results to guide decisions about food, physical activity, and medicines. Ask your health care team how often you should check your blood glucose level.
Protect your kidneys by keeping your blood glucose under control.
Control your blood pressure
Blood pressure is the force of your blood against the wall of your blood vessels. High blood pressure makes your heart work too hard. It can cause heart attack, stroke, and kidney disease.
Your health care team will also work with you to help you set and reach your blood pressure goal. The blood pressure goal for most people with diabetes is below 140/90 mm Hg. Ask your health care team what your goal should be.
Protect your kidneys by keeping your blood pressure under control.
Medicines that lower blood pressure can also help slow kidney damage. Two types of blood pressure medicines, ACE inhibitors and ARBs, play a special role in protecting your kidneys. Each has been found to slow kidney damage in people with diabetes who have high blood pressure and DKD. The names of these medicines end in –pril or –sartan. ACE inhibitors and ARBs are not safe for women who are pregnant.
Develop or maintain healthy lifestyle habits
Healthy lifestyle habits can help you reach your blood glucose and blood pressure goals. Following the steps below will also help you keep your kidneys healthy:
Stop smoking.
Work with a dietitian to develop a diabetes meal plan and limit salt and sodium.
Make physical activity part of your routine.
Stay at or get to a healthy weight.
Get enough sleep. Aim for 7 to 8 hours of sleep each night.
Medicines may be an important part of your treatment plan. Your health care professional will prescribe medicine based on your specific needs. Medicine can help you meet your blood glucose and blood pressure goals. You may need to take more than one kind of medicine to control your blood pressure.
Talk to your health care professional or pharmacist about all of the medicines you take, including over-the-counter medicines.
How can I cope with the stress of managing my diabetes?
Managing diabetes isn’t always easy. Feeling stressed, sad, or angry is common when you are living with diabetes. You may know what to do to stay healthy but may have trouble sticking with your plan over time. Long-term stress can raise your blood glucose and blood pressure, but you can learn ways to lower your stress. Try deep breathing, gardening, taking a walk, doing yoga, meditating, doing a hobby, or listening to your favorite music. Learn more about healthy ways to cope with stress.
Does diabetic kidney disease get worse over time?
Kidney damage from diabetes can get worse over time. However, you can take steps to keep your kidneys healthy and help slow kidney damage to prevent or delay kidney failure. Kidney failure means that your kidneys have lost most of their ability to function—less than 15 percent of normal kidney function. However, most people with diabetes and kidney disease don’t end up with kidney failure.
If your kidneys become damaged as a result of diabetes, learn how to manage kidney disease.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank: Ian de Boer, MD, MS, Associate Professor, Division of Nephrology, University of Washington, Associate Director, Kidney Research Institute
Diabetes management and treatment is expensive. According to the American Diabetes Association (ADA), the average cost of health care for a person with diabetes is $13,741 a year—more than twice the cost of health care for a person without diabetes.1
Many people who have diabetes need help paying for their care. For those who qualify, a variety of government and nongovernment programs can help cover health care expenses. This publication is meant to help people with diabetes and their family members find and access such resources.
1American Diabetes Association. Economic costs of diabetes in the U.S. in 2012. Diabetes Care. 2013;36(4):1033–1046.
What is health insurance?
Health insurance helps pay for medical care, including the cost of diabetes care. Health insurance options include the following:
private health insurance, which includes group and individual health insurance
government health insurance, such as Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), TRICARE, and veterans’ health care programs
Starting in 2014, the Affordable Care Act (ACA) prevents insurers from denying coverage or charging higher premiums to people with preexisting conditions, such as diabetes. The ACA also requires most people to have health insurance or pay a fee. Some people may be exempt from this fee. Read more about the ACA at HealthCare.gov or call 1–800–318–2596, TTY 1–855–889–4325.
Key Terms
Some terms listed here have many meanings; only those meanings that relate to the financial and medical aspects of diabetes and its management and treatment are included.
affiliation period: a period of time that must pass before health insurance coverage provided by a health maintenance organization (HMO) becomes effective.
coinsurance: an amount a person may still need to pay after a deductible for health care. The amount is most often a percent, such as 20 percent.
coordination period: if a person has more than one health plan, a coordination period is used to figure out which plan pays first and for how long. For example, if a person has an employer group plan and Medicare, the employer group plan is the first payer for the first 30 months the person is eligible for Medicare.
copay (or copayment): an amount a person may have to pay for health care. A copay is often a set fee. A person might pay $10 or $20 for a health care provider’s visit or prescription.
deductible: an amount a person must pay for health care or prescriptions before the health plan(s) will pay.
network: a group of health care providers that gives members a discount. Some plans pay for health care and prescriptions only if received from a network provider.
out of network: health care providers who are not in a plan’s network. In some health plans, health care and prescriptions cost more if received from these providers.
premium: an amount a person must pay periodically—monthly or quarterly—for Medicare, other health plan, or drug plan coverage.
primary payer: the health plan that pays medical bills first, before bills can be sent to a secondary payer.
secondary payer: the health plan that pays medical bills second, after the primary payer has paid its portion.
social worker: a person with special training to help people solve problems in their daily lives, especially people with disabilities or low incomes. A social worker may help with financial and employment issues.
waiting period: the time that must pass before coverage can become effective for an employee or a dependent, who is otherwise eligible for coverage under a job-based health plan.
What is private health insurance?
Insurance companies sell private health insurance plans. Two types of private health insurance are
Group health insurance. People may be eligible to purchase group health insurance through their employer or union or through a family member’s employer or union. Other organizations, such as professional or alumni organizations, may also offer group health insurance.
Individual health insurance. People may purchase individual health insurance for themselves and their families. The website HealthCare.gov provides information about individual insurance plans. The website also provides a search function, called the Health Insurance Marketplace, to find health insurance options by state. Depending on their income and family size, some people may qualify for lower-cost premiums through the Health Insurance Marketplace. People can select or change individual health insurance plans during the open enrollment period each year. HealthCare.gov lists open enrollment period dates. The website also provides information about life events that may allow people to enroll outside the open enrollment period.
Employers may have a waiting period before an employee and his or her family members can enroll in the company health plan. Under the ACA, the waiting period can be no longer than 90 days. Certain health plans called health maintenance organizations (HMOs) may have an affiliation period—a time that must pass before health insurance coverage becomes effective. An affiliation period can be no longer than 3 months.
The ACA expanded coverage of preventive services. For example, adults with sustained high blood pressure may have access to diabetes screening at no cost. Adults and children may have access to obesity screening and counseling at no cost.
Each state’s insurance regulatory office, sometimes called the state insurance department or commission, provides more information about health insurance laws. This office can also help identify an insurance company that offers individual coverage. The National Association of Insurance Commissioners’ website, www.naic.org/state_web_map.htm , provides a membership list with contact information and a link to the website for each state’s insurance regulatory office.
Keeping Group Health Insurance after Leaving a Job
When leaving a job, a person may be able to continue the group health insurance provided by his or her employer for up to 18 months under a federal law called the Consolidated Omnibus Budget Reconciliation Act, or COBRA. Although people pay more for group health insurance through COBRA than they did as employees, group coverage may be cheaper than individual coverage. People who have a disability before becoming eligible for COBRA or who are determined by the Social Security Administration to be disabled within the first 60 days of COBRA coverage may be able to extend COBRA coverage an additional 11 months, for up to 29 months of coverage. COBRA may also cover young adults who were insured under a parent’s policy after they have reached the age limit and are trying to obtain their own insurance.
If a person doesn’t qualify for coverage or if COBRA coverage has expired, other options may be available:
Some states require employers to offer conversion policies, in which people stay with their insurance company and buy individual coverage.
Some professional and alumni organizations offer group coverage for members.
Some insurance companies offer short-term stopgap policies designed for people who are between jobs. However, these policies may not meet ACA requirements. For example, they may not cover preexisting conditions.
People can purchase individual health insurance policies.
Each state’s insurance regulatory office can provide more information about these and other options. Information about consumer health plans is also available at the U.S. Department of Labor’s website at www.dol.gov/dol/topic/health-plans/consumerinfhealth.htm.
What is Medicare?
Medicare is a federal health insurance program that pays health care costs for eligible people who are
age 65 or older
under age 65 with certain disabilities
of any age with end-stage renal disease—total and permanent kidney failure that requires a kidney transplant or blood-filtering treatments called dialysis
What health plans does Medicare offer?
Medicare has four parts:
Part A (hospital insurance) covers inpatient care, skilled nursing home residence, hospice care, and home health care. Part A has no premium for those who have paid enough Medicare taxes. A premium is an amount a person must pay periodically—monthly or quarterly—for Medicare, other health plan, or drug plan coverage. Part A does have a deductible, an amount a person must pay for health care or prescriptions before the health plan will pay. A person must pay a daily amount for hospital stays that last longer than 60 days.
Part B (medical insurance) covers services from health care providers, outpatient care, home health care, durable medical equipment, and some preventative services. Part B has a monthly premium based on a person’s income. Rates change each year. After a person pays the deductible each year, Part B pays 80 percent for most covered services as a primary payer. The billing staff of the service provider—hospital or clinic—can calculate how much a person will owe.
Part C (Medicare Advantage Plans) are part of Medicare and are sometimes called MA Plans. Medicare must approve Medicare Advantage Plans. Each Medicare Advantage Plan must cover Part A and Part B services and may cover other services, too. Medicare Advantage Plans may have Part D prescription coverage. If not, a person can buy a Part D plan separately. Medicare Advantage Plans are not all the same. A person who is thinking of choosing a Medicare Advantage Plan should ask about the rules of the plan. The rules may specify which health care providers or hospitals a person may use. The plan may require a referral from a primary care provider to see a specialist. The plan may not cover medical expenses incurred during travel. How much a person has to pay out-of-pocket each year will vary by plan. People who have a Medicare Advantage Plan cannot have a Medigap plan to help pay out of-pocket costs. See the section on Medigap.
Four types of Medicare Advantage Plans are available:
HMOs
preferred provider organizations (PPOs)
private fee for service plans
special needs plans for certain groups
Part D (prescription drug coverage) has a premium and covers some medications. Private insurance companies offer different Part D plans approved by Medicare. Costs and coverage vary by plan. A person who has few assets and earns less than 150 percent of the federal poverty level may qualify for extra help to pay Part D premiums and medication costs. People can apply for this help by calling the Social Security Administration, visiting www.socialsecurity.gov to apply online, visiting their local Social Security office, or contacting their state medical assistance (Medicaid) office. People can find the current-year guidelines at www.aspe.hhs.gov/poverty or by calling Social Security at 1–800–772–1213, TTY 1–800–325–0778. People can find information and applications for Part D plans at www.medicare.gov. A person can also apply for Part D with an insurance company that sells one of these plans.
Other Medicare health plans are for certain groups, such as frail people living in the community and people with multiple chronic illnesses, and include hospital and medical coverage. Some pay for prescribed medications, too. State health insurance programs—called Medicaid—partially finance and administer these services. The plans include the following:
Medicare Cost Plans are HMOs, like the ones offered as Medicare Advantage plans, only out-of-network providers are paid as if the policyholder had Original Medicare. Original Medicare is Medicare Part A and Part B.
Program of All-Inclusive Care for the Elderly (PACE) combines medical, social, and long-term care services for frail people who live and get health care in the community.
Medicare Innovation Projects are special projects that test improvements in Medicare coverage, payment, and quality of care.
Read more about Medicare Cost Plans and Demonstration or Pilot Programs on the state Medicaid website at www.medicaid.gov or call 1–800–MEDICARE (1–800–633–4227). State Medicaid offices can provide more information about PACE. See the section on Medicaid.
Does Medicare cover diabetes services and supplies?
Medicare helps pay for the diabetes services, supplies, and equipment listed below and for some preventive services for people who are at risk for diabetes. However, coinsurance or deductibles may apply. A person must have Medicare Part B or Medicare Part D to receive these covered services and supplies.
Medicare Part B helps pay for
diabetes screening tests for people at risk of developing diabetes
diabetes self-management training
diabetes supplies such as glucose monitors, test strips, and lancets
insulin pumps and insulin if used with an insulin pump
counseling to help people who are obese lose weight
flu and pneumonia shots
foot exams and treatment for people with diabetes
eye exams to check for glaucoma and diabetic retinopathy
medical nutrition therapy services for people with diabetes or kidney disease, when referred by a health care provider
therapeutic shoes or inserts, in some cases
Medicare Part D helps pay for
diabetes medications
insulin, excluding insulin used with an insulin pump
diabetes supplies such as needles and syringes for injecting insulin
People who are in a Medicare Advantage Plan or other Medicare health plan should check their plan’s membership materials and call for details about how the plan provides the diabetes services, supplies, and medications covered by Medicare.
Where can a person find more information about Medicare?
A person can find more information about Medicare by
visiting the Medicare website
calling 1–800–MEDICARE
Medicare website. Read more about Medicare at www.medicare.gov, the official U.S. Government website for people with Medicare. The website has a full range of information about Medicare, including free publications such as Medicare & You, which is the official Government handbook about Medicare, and Medicare Basics—A Guide for Families and Friends of People with Medicare.
Through the Medicare website, people can also
find out if they are eligible for Medicare and when they can enroll
learn about their Medicare health plan options
find out what Medicare covers
find a Medicare Prescription Drug Plan
compare Medicare health plan options in their area
find a health care provider who participates in Medicare
get information about the quality of care provided by hospitals, home health agencies, and dialysis facilities
Calling Medicare. Calling 1–800–MEDICARE (1–800–633–4227) is another way to get help with Medicare questions, order free publications, and more. Help is available 24 hours a day, every day, and is available in English, Spanish, and other languages. TTY users should call 1–877–486–2048.
Access Personal Medicare Information
People who enroll in Medicare can register with www.MyMedicare.gov, a secure online service, and use the site to access their personal Medicare information at any time. People can view their claims and order history, and see a description of covered preventive services.
What is Medigap?
A Medigap plan, also known as a Medicare supplement plan, can help pay what Original Medicare does not pay for covered services. Insurance companies sell Medigap coverage. People who have a Medicare Advantage plan cannot also have a Medigap plan. A person can buy a Medigap policy from any insurance company licensed to sell the policy in the person’s home state.
For people who are 65 and older, federal law says that in the first 6 months a person has Part B, companies cannot deny an application or limit payment for anything Original Medicare covers. Some states make insurance companies sell at least one Medigap coverage plan to those under 65 with Medicare. State insurance offices can explain the plans in their state. Find local offices on a map at www.naic.org/state_web_map.htm.
What other federal programs can help?
The following federal programs can provide more resources for people with diabetes:
Department of Veterans Affairs (VA)
TRICARE
The Indian Health Service
The Hill-Burton Free and Reduced-Cost Health Care Program
Bureau of Primary Health Care
Social Security Administration
Social Security Disability Insurance (SSDI)
Supplemental Security Income (SSI)
Women, Infants, and Children (WIC)
The VA runs hospitals and clinics that serve veterans who have service-related health problems or who simply need financial aid. Read more at www.va.gov/healthbenefits/online or call 1–877–222–8387.
TRICARE—the health care program serving uniformed service members, retirees, and their families worldwide—is available to people who are
active duty service members
military retirees
family members of an active duty service member or a military retiree
members of the National Guard/Reserves on active duty for 30 days
family members of someone who is in the National Guard/Reserves on active duty for 30 days
TRICARE for Life is a specific TRICARE plan that offers secondary coverage for people who have Medicare Part A and Part B. Read more about TRICARE and access phone numbers for its four regions at www.tricare.mil .
The Indian Health Service may help members of federally recognized American Indian or Alaska Native tribes. Read more on the Indian Health Service website at www.IHS.gov. American Indians or Alaska Natives may also be eligible for help from public, private, and state programs.
The Hill-Burton Free and Reduced-Cost Health Care Program can help people who are uninsured and need help with the cost of hospital care. Although the program originally provided hospitals with federal grants for modernization, today it provides free or reduced-fee medical services to people with low incomes. The U.S. Department of Health and Human Services administers the program. Read more at www.hrsa.gov/gethealthcare/affordable/hillburton or call 1–800–638–0742 (1–800–492–0359 in Maryland).
The Bureau of Primary Health Care, a service of the Health Resources and Services Administration (HRSA), offers primary and preventive health care to medically underserved populations through community health centers. For people with no insurance, the Bureau bases fees for care on family size and income. To find local health centers, call 1–888–ASK–HRSA (1–888–275–4772) and ask for a directory, or visit http://findahealthcenter.hrsa.gov.
The Social Security Administration can provide information about eligibility for Medicare. People can contact the agency at 1–800–772–1213, visit the agency website at www.socialsecurity.gov, or check with their local Social Security office to learn if they are eligible for Medicare.
The Social Security Administration also provides the following programs:
SSDI is a federal insurance plan that pays a monthly amount to people who cannot work. People earn SSDI work credits when they pay Social Security taxes. A person must have enough credits based on age to qualify. Then, if an illness or injury prohibits a person from working for at least a year, SSDI payments may be an option. A chart shows how many work credits a person needs at www.socialsecurity.gov/retire2/credits3.htm.
SSI is a federal safety net program that pays a monthly amount to disabled children and adults who earn little and have few assets. A person who gets SSI may be able to get food stamps and Medicaid, too.
Read more about both SSDI and SSI and how to apply at www.ssa.gov or by calling 1–800–772–1213, TTY 1–800–325–0778.
WIC provides the following services to low-income pregnant, breastfeeding, and postpartum women, as well as infants and children up to age 5 who are at nutritional risk:
supplemental foods
health care referrals
nutrition education
breastfeeding information
The U.S. Department of Agriculture administers the program. Applicants must meet residential, financial need, and nutrition risk criteria to be eligible for assistance. Having gestational diabetes is considered a medically based nutrition risk and would qualify a woman for assistance through the WIC program if she meets the financial need requirements and has lived in a particular state the required amount of time. The WIC website provides a page of contact information for each state and for American Indian and Alaska Native tribes. Read more at www.fns.usda.gov/wic or call the WIC’s national headquarters at 703–305–2062.
What are Medicaid and the Children’s Health Insurance Program?
Medicaid is a state health insurance program for those with low incomes and few assets. Each state runs its own program. The Federal Government requires that Medicaid programs cover a specific set of services; however, states can choose to cover more services in addition to the ones required. A person may have Medicaid alone or Medicare and Medicaid. If a person has both types of coverage, Medicare pays first and Medicaid pays second. Medicaid may pay for things Medicare does not. A person can apply for Medicaid at a city or county department of social services office. The state medical assistance (Medicaid) office can help people find out whether they qualify for Medicaid and can provide more information about Medicaid programs. A social worker can also explain a state’s Medicaid program and help a person apply.
To contact a state Medicaid office, people can
search for Medicaid information for a state at www.medicaid.gov or call 1–877–267–2323
search online or check the government pages of the phone book for the local department of human services or department of social services
CHIP gives free or low-cost Medicaid to children whose parents earn too much for Medicaid, though not enough to pay for a health plan. CHIP may also provide assistance to parents. CHIP is a federal and state program. Read more at www.insurekidsnow.gov or call 1–877–543–7669.
What other state programs can help?
The following state programs can provide more resources for people with diabetes:
Medicare Savings Programs
State Health Insurance Assistance Programs (SHIPs)
State Pharmaceutical Assistance Programs (SPAPs)
Medicare Savings Programs. Some states may pay Medicare premiums, deductibles, and coinsurance if a person has low income and few assets. A city or county department of social services can determine whether a person is eligible.
SHIP. SHIPs get money from the Federal Government to give free health insurance advice to those with Medicare. SHIP counselors can help people choose a Medicare health plan or a Medicare Prescription Drug Plan. A person can find a SHIP counselor at www.shiptalk.org . A person who needs more health insurance should talk with a SHIP counselor or a social worker.
SPAP. Several states have SPAPs that help certain people pay for prescription drugs. Each SPAP makes its own rules about how to provide drug coverage to its members. Read more about each state’s SPAP at www.medicare.gov/pharmaceutical-assistance-program/state-programs.aspx, or call Medicare or the state’s SHIP.
What local resources can help?
Many local governments have public health departments that can help people who need medical care. The local county or city government’s health and human services office can provide further information. Local resources such as the following charitable groups may offer financial help for some expenses related to diabetes:
Lions Clubs International can help with vision care. Visit www.lionsclubs.org .
Rotary International clubs provide humanitarian and educational assistance. Visit www.rotary.org .
Elks clubs provide charitable activities that benefit youth and veterans. Visit www.elks.org .
Kiwanis International clubs conduct service projects to help children and communities. Visit www.kiwanis.org .
In many areas, nonprofit or special-interest groups, such as those listed above, can sometimes provide financial assistance or help with fundraising. Religious organizations also may offer assistance. In addition, some local governments may have special trusts set up to help people in need. The local library or local city or county government’s health and human services office may provide more information about such groups.
The NIDDK gathered information from various agencies and organizations to provide the most comprehensive and helpful information possible. Changes may occur in these programs from the time the NIDDK published this information. Please contact each organization directly for the most up-to-date information. The NIDDK welcomes corrections and updates to the information on this page. Please send updates to healthinfo@niddk.nih.gov.
How can a person save money on diabetes medications and medical supplies?
People should talk with their health care providers if they have problems paying for diabetes medications. Some people do not fill prescriptions or take less medication than what a provider prescribes in order to save money; however, health care providers advise against taking less than the prescribed amount of medication. Less expensive generic medications for diabetes, blood pressure, and cholesterol are available. If a health care provider prescribes medications that a person cannot afford, the person should ask the health care provider about cheaper alternatives.
Health care providers may also be able to assist people who need help paying for their medications and diabetes testing supplies, such as glucose test strips, by providing free samples or referring them to local programs. Drug companies that sell insulin or diabetes medications often have patient assistance programs. Each patient assistance program has its own eligibility criteria.
The websites below provide links to programs that can help patients determine if they qualify for the different types of assistance and find free or low-cost health care. People can also search these websites for needed diabetes testing supplies by using keywords such as “glucose test strips” or the names of specific diabetes medications.
The Partnership for Prescription Assistance website at www.PPARx.org lists more than 475 programs that help pay for medications. The drug companies that produce medications provide many of these programs. People can find programs and apply for help by calling 1–888–477–2669.
NeedyMeds is a nonprofit group that helps people find programs that help pay for medications. The NeedyMeds website at www.NeedyMeds.org allows the user to search a list of programs by medication or manufacturer name. Some of the forms to apply are online.
RxAssist has a website at www.rxassist.org that provides information about drug company programs, state programs, discount drug cards, copay help, and more.
Rx Outreach is a nonprofit pharmacy that provides affordable medications to people in need. The Rx Outreach website at www.rxoutreach.org provides information about the medications offered and how to apply.
The National Council on Aging provides benefit information for seniors with limited income and resources at www.benefitscheckup.org .
HRSA offers a free nylon filament—similar to a bristle on a hairbrush—to check feet for nerve damage. Order the filament, with instructions for use, at www.hrsa.gov/leap or call 1–888–ASK–HRSA (1–888–275–4772, TTY 1–877–489–4772).
Also, some programs for the homeless may be able to provide help. A person can contact a local homeless shelter for more information about how to obtain free medications and medical supplies. People can access the number or location of the nearest homeless shelter online or in the phone book under “Human Service Organizations” or “Social Service Organizations.”
Where can a person find help paying for prosthetic care?
People who have had an amputation may need assistance in paying their rehabilitation expenses and the cost of a prosthesis. The following organizations provide financial assistance or information about finding resources for people who need prosthetic care:
Amputee Coalition 900 East Hill Avenue, Suite 290 Knoxville, TN 37915 Phone: 1–888–AMP–KNOW (1–888–267–5669) TTY: 865–525–4512 Internet: www.amputee-coalition.org
Limbs for Life Foundation 218 East Main Street Oklahoma City, OK 73104 Phone: 1-888-235-5462 or 405-605-5462 Fax: 405-843-5123 Email: admin@limbsforlife.org Internet: www.limbsforlife.org
Where can a person find help paying for kidney dialysis and transplantation?
Kidney failure, also called end-stage renal disease, is a complication of diabetes. People of any age with kidney failure can get Medicare if they meet certain criteria. More information is provided in the NIDDK health topic, Financial Help for Treatment of Kidney Failure.
What services are available for children attending school or adults attending college?
College students who have diabetes-related disabilities may face both the costs of tuition and additional expenses. These costs may include special equipment and disability-related medical expenses not covered by insurance. Some special equipment and support services may be available at the educational institution, or through community organizations, the state vocational rehabilitation agency, or specific disability organizations.
The HEATH Resource Center, an online clearinghouse on postsecondary education for individuals with disabilities, offers information about sources of financial aid. Contact the clearinghouse at
The George Washington University Graduate School of Education and Human Development HEATH Resource Center at the National Youth Transitions Center 2134 G Street NW, Suite 308 Washington, D.C. 20052–0001 Email: AskHEATH@gwu.edu Internet: www.heath.gwu.edu
What is assistive technology and what organizations might provide assistance?
Assistive technology is any device that assists, adapts, or helps to rehabilitate someone with a disability so he or she may function more safely, effectively, and independently at home, at work, and in the community. Assistive technology may include
computers with features that make them accessible to people with disabilities
adaptive equipment, such as wheelchairs
bathroom modifications, such as grab bars or shower seats
The following organizations may be able to provide information, awareness, and training in the use of technology to assist people with disabilities:
Alliance for Technology Access 1119 Old Humboldt Road Jackson, TN 38305 Phone: 1–800–914–3017 or 731–554–5ATA (731–554–5282) TTY: 731–554–5284 Fax: 731–554–5283 Email: atainfo@ataccess.org
National Assistive Technology Technical Assistance Partnership 1700 North Moore Street, Suite 1540 Arlington, VA 22209–1903 Phone: 703–524–6686 Fax: 703–524–6630 TTY: 703–524–6639 Email: resnaTA@resna.org Internet: www.resnaprojects.org/nattap
Diabetes management and treatment is expensive. Many people who have diabetes need help paying for their care. For those who qualify, a variety of government and nongovernment programs can help cover health care expenses.
Health insurance helps pay for medical care, including the cost of diabetes care. Health insurance options include private health insurance and government health insurance.
Insurance companies sell private health insurance plans. Two types of private health insurance are group health insurance and individual health insurance.
Medicare is a federal health insurance program that pays health care costs for eligible people who are age 65 or older, under age 65 with certain disabilities, or of any age with end-stage renal disease.
Medicaid is a state health insurance program for those with low incomes and few assets. Each state runs its own program.
The Children’s Health Insurance Program (CHIP) gives free or low-cost Medicaid to children whose parents earn too much for Medicaid, though not enough to pay for a health plan.
Many local governments have public health departments that can help people who need medical care. Local resources such as charitable groups may offer financial help for some expenses related to diabetes.
People should talk with their health care providers if they have problems paying for diabetes medications. Less expensive generic medications for diabetes, blood pressure, and cholesterol are available. If a health care provider prescribes medications that a person cannot afford, the person should ask the health care provider about cheaper alternatives.
Health care providers may also be able to assist people who need help paying for their medications and diabetes testing supplies, such as glucose test strips, by providing free samples or referring them to local programs. Drug companies that sell insulin or diabetes medications often have patient assistance programs.
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you? Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open? Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank: Thomas Dudley, M.S., R.N., Centers for Medicare & Medicaid Services
Taking insulin or other diabetes medicines is often part of treating diabetes. Along with healthy food choices and physical activity, medicine can help you manage the disease. Some other treatment options are also available.
What medicines might I take for diabetes?
The medicine you take will vary by your type of diabetes and how well the medicine controls your blood glucose levels, also called blood sugar. Other factors, such as your other health conditions, medication costs, and your daily schedule may play a role in what diabetes medicine you take.
Type 1 diabetes
If you have type 1 diabetes, you must take insulin because your body no longer makes this hormone. You will need to take insulin several times during the day, including with meals. You also could use an insulin pump, which gives you small, steady doses throughout the day.
Type 2 diabetes
Some people with type 2 diabetes can manage their disease by making healthy food choices and being more physically active. Many people with type 2 diabetes need diabetes medicines as well. These medicines may include diabetes pills or medicines you inject under your skin, such as insulin. In time, you may need more than one diabetes medicine to control your blood glucose. Even if you do not take insulin, you may need it at special times, such as during pregnancy or if you are in the hospital.
Gestational diabetes
If you have gestational diabetes, you should first try to control your blood glucose level by making healthy food choices and getting regular physical activity. If you can’t reach your blood glucose target, your health care team will talk with you about diabetes medicines, such as insulin or the diabetes pill metformin, that may be safe for you to take during pregnancy. Your health care team may start you on diabetes medicines right away if your blood glucose is very high.
No matter what type of diabetes you have, taking diabetes medicines every day can feel like a burden sometimes. You may also need medicines for other health problems, such as high blood pressure or high cholesterol, as part of your diabetes care plan. View resources that may help you manage your medication plan.
What are the different types of insulin?
Several types of insulin are available. Each type starts to work at a different speed, known as “onset,” and its effects last a different length of time, known as “duration.” Most types of insulin reach a peak, which is when they have the strongest effect. Then the effects of the insulin wear off over the next few hours or so.
The chart above gives averages. Follow your doctor’s advice on when and how to take your insulin. Your doctor might also recommend premixed insulin, which is a mix of two types of insulin. Some types of insulin cost more than others, so talk with your doctor about your options if you're concerned about cost. Read about financial help for diabetes care.
What are the different ways to take insulin?
The way you take insulin may depend on your lifestyle, insurance plan, and preferences. You may decide that needles are not for you and prefer a different method. Talk with your doctor about the options and which is best for you. Most people with diabetes use a needle and syringe, pen, or insulin pump. Inhalers, injection ports, and jet injectors are less common.
Needle and syringe
You’ll give yourself insulin shots using a needle and syringe. You will draw up your dose of insulin from the vial, or bottle, into the syringe. Insulin works fastest when you inject it in your belly, but you should rotate spots where you inject insulin. Other injection spots include your thigh, buttocks, or upper arm. Some people with diabetes who take insulin need two to four shots a day to reach their blood glucose targets. Others can take a single shot.
Insulin shots involve drawing insulin from a vial into a syringe and then injecting it under your skin.
Pen
An insulin pen looks like a pen but has a needle for its point. Some insulin pens come filled with insulin and are disposable. Others have room for an insulin cartridge that you insert and then replace after use. Insulin pens cost more than needles and syringes but many people find them easier to use.
An insulin pen is a convenient way to take insulin
Pump
An insulin pump is a small machine that gives you small, steady doses of insulin throughout the day. You wear one type of pump outside your body on a belt or in a pocket or pouch. The insulin pump connects to a small plastic tube and a very small needle. You insert the needle under your skin and it stays in place for several days. Insulin then pumps from the machine through the tube into your body 24 hours a day. You also can give yourself doses of insulin through the pump at mealtimes. Another type of pump has no tubes and attaches directly to your skin, such as a self-adhesive pod.
Insulin pumps deliver insulin 24 hours a day.
Inhaler
Another way to take insulin is by breathing powdered insulin from an inhaler device into your mouth. The insulin goes into your lungs and moves quickly into your blood. Inhaled insulin is only for adults with type 1 or type 2 diabetes.
Injection port
An injection port has a short tube that you insert into the tissue beneath your skin. On the skin’s surface, an adhesive patch or dressing holds the port in place. You inject insulin through the port with a needle and syringe or an insulin pen. The port stays in place for a few days, and then you replace the port. With an injection port, you no longer puncture your skin for each shot—only when you apply a new port.
Jet injector
This device sends a fine spray of insulin into the skin at high pressure instead of using a needle to deliver the insulin.
What oral medicines treat type 2 diabetes?
You may need medicines along with healthy eating and physical activity habits to manage your type 2 diabetes. You can take many diabetes medicines by mouth. These medicines are called oral medicines.
Most people with type 2 diabetes start medical treatment with metformin pills. Metformin also comes as a liquid. Metformin lowers the amount of glucose that your liver makes and helps your body use insulin better. This drug may help you lose a small amount of weight.
Other oral medicines act in different ways to lower blood glucose levels. You may need to add another diabetes medicine after a while or use a combination treatment. Combining two or three kinds of diabetes medicines can lower blood glucose levels more than taking just one.
Read about different kinds of diabetes medicines from the Food and Drug Administration (FDA).
What other injectable medicines treat type 2 diabetes?
Besides insulin, other types of injected medicines are available. These medicines help keep your blood glucose level from going too high after you eat. They may make you feel less hungry and help you lose some weight. Other injectable medicines are not substitutes for insulin. Learn more about noninsulin injectable medicines.
What should I know about side effects of diabetes medicines?
Side effects are problems that result from a medicine. Some diabetes medicines can cause hypoglycemia, also called low blood glucose, if you don’t balance your medicines with food and activity.
Ask your doctor whether your diabetes medicine can cause hypoglycemia or other side effects, such as upset stomach and weight gain. Take your diabetes medicines as your health care professional has instructed you, to help prevent side effects and diabetes problems.
Do I have other treatment options for my diabetes?
When medicines and lifestyle changes are not enough to manage your diabetes, a less common treatment may be an option. Other treatments include bariatric surgery for certain people with type 1 or type 2 diabetes, and an "artificial pancreas" and pancreatic islet transplantation for some people with type 1 diabetes.
Bariatric surgery
Also called weight-loss surgery or metabolic surgery, bariatric surgery may help some people with obesity and type 2 diabetes lose a large amount of weight and regain normal blood glucose levels. Some people with diabetes may no longer need their diabetes medicine after bariatric surgery. Whether and for how long blood glucose levels improve seems to vary by the patient, type of weight-loss surgery, and amount of weight the person loses. Other factors include how long someone has had diabetes and whether or not the person uses insulin.1
Recent research suggests that weight-loss surgery also may help improve blood glucose control in people with type 1 diabetes who are obese.2
Researchers are studying the long-term results of bariatric surgery in people with type 1 and type 2 diabetes.
Artificial Pancreas
The NIDDK has played an important role in developing “artificial pancreas” technology. An artificial pancreas replaces manual blood glucose testing and the use of insulin shots or a pump. A single system monitors blood glucose levels around the clock and provides insulin or a combination of insulin and a second hormone, glucagon, automatically. The system can also be monitored remotely, for example by parents or medical staff.
In 2016, the FDA approved a type of artificial pancreas system called a hybrid closed-loop system. This system tests your glucose level every 5 minutes throughout the day and night, and automatically gives you the right amount of insulin.
You still need to manually adjust the amount of insulin the pump delivers at mealtimes. But, the artificial pancreas may free you from some of the daily tasks needed to keep your blood glucose stable—or help you sleep through the night without the need to wake and test your glucose or take medicine.
The hybrid closed-loop system is expected to be available in the U.S. in 2017. Talk with your health care provider about whether this system might be right for you.
The NIDDK has funded several important studies on different types of artificial pancreas devices to better help people with type 1 diabetes manage their disease. The devices may also help people with type 2 diabetes and gestational diabetes.
Pancreatic islet transplantation
Pancreatic islet transplantation is an experimental treatment for poorly controlled type 1 diabetes. Pancreatic islets are clusters of cells in the pancreas that make the hormone insulin. In type 1 diabetes, the body’s immune system attacks these cells. A pancreatic islet transplant replaces destroyed islets with new ones that make and release insulin. This procedure takes islets from the pancreas of an organ donor and transfers them to a person with type 1 diabetes. Because researchers are still studying pancreatic islet transplantation, the procedure is only available to people enrolled in research studies. Learn more about islet transplantation studies.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Checking your blood sugar, also called blood glucose, is an important part of diabetes care. This tip sheet tells you:
why it helps you to know your blood sugar numbers
how to check your blood sugar levels
what are target blood sugar levels
what to do if your levels are too low or too high
how to pay for these tests
?Why do I need to know my blood sugar numbers?
Your blood sugar numbers show how well your diabetes is managed. And managing your diabetes means that you have less chance of having serious health problems, such as kidney disease and vision loss.
As you check your blood sugar, you can see what makes your numbers go up and down. For example, you may see that when you are stressed or eat certain foods, your numbers go up. And, you may see that when you take your medicine and are active, your numbers go down. This information lets you know what is working for you and what needs to change.
How is blood sugar measured?
There are two ways to measure blood sugar.
Blood sugar checks that you do yourself. These tell you what your blood sugar level is at the time you test.
The A1C (A-one-C) is a test done in a lab or at your provider’s office. This test tells you your average blood sugar level over the past 2 to 3 months.
How do I check my blood sugar?
You use a blood glucose meter to check your blood sugar. This device uses a small drop of blood from your finger to measure your blood sugar level. You can get the meter and supplies in a drug store or by mail.
Read the directions that come with your meter to learn how to check your blood sugar. Your health care team also can show you how to use your meter. Write the date, time, and result of the test in your blood sugar record. Take your blood sugar record and meter to each visit and talk about your results with your health care team.
What are target blood sugar levels for people with diabetes?
A target is something that you aim for or try to reach. Your health care team may also use the term goal. People with diabetes have blood sugar targets that they try to reach at different times of the day. These targets are:
Right before your meal: 80 to 130
Two hours after the start of the meal: Below 180
Talk with your health care team about what blood sugar numbers are right for you.
How often should I check my blood sugar?
The number of times that you check your blood sugar will depend on the type of diabetes that you have and the type of medicine you take to treat your diabetes. For example, people who take insulin may need to check more often than people who do not take insulin. Talk with your health care team about how often to check your blood sugar.
The common times for checking your blood sugar are when you first wake up (fasting), before a meal, 2 hours after a meal, and at bedtime. Talk with your health care team about what times are best for you to check your blood sugar.
What should I do if my blood sugar gets too high?
High blood sugar is also called hyperglycemia (pronounced hye-per-gly-see-mee-uh). It means that your blood sugar level is higher than your target level or over 180. Having high blood sugar levels over time can lead to long-term, serious health problems.
If you feel very tired, thirsty, have blurry vision, or need to pee more often, your blood sugar may be high.
Check your blood sugar and see if it is above your target level or over 180. If it is too high, one way to lower it is to drink a large glass of water and exercise by taking a brisk walk. Call your health care team if your blood sugar is high more than 3 times in 2 weeks and you don’t know why.
What should I do if my blood sugar gets too low?
Low blood sugar is also called hypoglycemia (pronounced hye-poh-gly-see-mee-uh). It means your blood sugar level drops below 70. Having low blood sugar is dangerous and needs to be treated right away. Anyone with diabetes can have low blood sugar. You have a greater chance of having low blood sugar if you take insulin or certain pills for diabetes.
Carry supplies for treating low blood sugar with you. If you feel shaky, sweaty, or very hungry, check your blood sugar. Even if you feel none of these things, but think you may have low blood sugar, check it.
If your meter shows that your blood sugar is lower than 70, do one of the following things right away:
chew 4 glucose tablets
drink 4 ounces of fruit juice
drink 4 ounces of regular soda, not diet soda or
chew 4 pieces of hard candy?
After taking one of these treatments, wait for 15 minutes, then check your blood sugar again. Repeat these steps until your blood sugar is 70 or above. After your blood sugar gets back up to 70 or more, eat a snack if your next meal is 1 hour or more away.
If you often have low blood sugar, check your blood sugar before driving and treat it if it is low.
What do I need to know about the A1C test?
The A1C test tells you and your health care team your average blood sugar level over the past 2 to 3 months. It also helps you and your team decide the type and amount of diabetes medicine you need.
What is a good A1C goal for me?
For many people with diabetes, the A1C goal is below 7. This number is different from the blood sugar numbers that you check each day. You and your health care team will decide on an A1C goal that is right for you.
How often do I need an A1C test?
You need to get an A1C test at least 2 times a year. You need it more often if:
your number is higher than your goal number
your diabetes treatment changes
How do I pay for these tests and supplies?
Medicare, Medicaid and most private insurance plans pay for the A1C test and some of the cost of supplies for checking your blood sugar. Check your plan or ask your health care team for help finding low cost or free supplies. Ask your health care team what to do if you run out of test strips. For more information about Medicare and diabetes, go to https://www.medicare.gov/.
What if I have trouble getting to my blood sugar goals?
There may be times when you have trouble reaching your blood sugar goals. This does not mean that you have failed. It means that you and your health care team should see if changes are needed. Call your health care team if your blood sugar is often too high or too low. Taking action will help you be healthy today and in the future.
John's Story
At each visit, John and his health care team look at his A1C test results, his blood glucose meter and his blood sugar record to see if his treatment is working. At today’s visit, John’s A1C and blood sugar numbers are too high. John and his health care team talk about what he can do to get closer to his A1C and blood sugar goals. John decides he will be more active. He will:?
increase his walking time to 30 minutes every day after dinner.
check his fasting blood sugar in the morning to see if being more active improves his blood sugar.
call his doctor in 1 month for a change in medicine if his blood sugar levels are still too high.
have his A1C tested again in 3 months to see if his new plan is working.?
Things to remember
Check your blood sugar as many times a day as your health care team suggests.
Have your A1C checked at least 2 times a year.
Keep a record of your blood sugar and A1C numbers.
Take your blood glucose meter and blood sugar record to your visit and show them to your health care team. Tell your health care team how you think you are doing.
Call your health care team if your blood sugar is often too high or too low.
Work with your health care team and decide what changes you need to make to reach your blood sugar goals.? Download a copy of the NDEP’s Managing and Monitoring Diabetes to learn more about managing diabetes.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank: Martha M. Funnell, M.S., R.N., C.D.E., Michigan Diabetes Research and Training Center
Hypoglycemia, also called low blood glucose or low blood sugar, occurs when the level of glucose in your blood drops below normal. For many people with diabetes, that means a level of 70 milligrams per deciliter (mg/dL) or less. Your numbers might be different, so check with your health care provider to find out what level is too low for you.
What are the symptoms of hypoglycemia?
Symptoms of hypoglycemia tend to come on quickly and can vary from person to person. You may have one or more mild-to-moderate symptoms listed in the table below. Sometimes people don’t feel any symptoms.
Severe hypoglycemia is when your blood glucose level becomes so low that you’re unable to treat yourself and need help from another person. Severe hypoglycemia is dangerous and needs to be treated right away. This condition is more common in people with type 1 diabetes.
Hypoglycemia Symptoms
Mild-to-Moderate
Severe
Shaky or jittery
Sweaty
Hungry
Headachy
Blurred vision
Sleepy or tired
Dizzy or lightheaded
Confused or disoriented
Pale
Uncoordinated
Irritable or nervous
Argumentative or combative
Changed behavior or personality
Trouble concentrating
Weak
Fast or irregular heart beat
Unable to eat or drink
Seizures or convulsions (jerky movements)
Unconsciousness
Some symptoms of hypoglycemia during sleep are
crying out or having nightmares
sweating enough to make your pajamas or sheets damp
feeling tired, irritable, or confused after waking up
What causes hypoglycemia in diabetes?
Hypoglycemia can be a side effect of insulin or other types of diabetes medicines that help your body make more insulin. Two types of diabetes pills can cause hypoglycemia: sulfonylureas and meglitinides. Ask your health care team if your diabetes medicine can cause hypoglycemia.
Although other diabetes medicines don’t cause hypoglycemia by themselves, they can increase the chances of hypoglycemia if you also take insulin, a sulfonylurea, or a meglitinide.
If you take insulin or some other diabetes medicines, your blood glucose level can drop too low.
What other factors contribute to hypoglycemia in diabetes?
If you take insulin or diabetes medicines that increase the amount of insulin your body makes—but don’t match your medications with your food or physical activity—you could develop hypoglycemia. The following factors can make hypoglycemia more likely:
Not eating enough carbohydrates (carbs)
When you eat foods containing carbohydrates, your digestive system breaks down the sugars and starches into glucose. Glucose then enters your bloodstream and raises your blood glucose level. If you don’t eat enough carbohydrates to match your medication, your blood glucose could drop too low.
Skipping or delaying a meal
If you skip or delay a meal, your blood glucose could drop too low. Hypoglycemia also can occur when you are asleep and haven’t eaten for several hours.
Increasing physical activity
Increasing your physical activity level beyond your normal routine can lower your blood glucose level for up to 24 hours after the activity.
Drinking too much alcohol without enough food
Alcohol makes it harder for your body to keep your blood glucose level steady, especially if you haven’t eaten in a while. The effects of alcohol can also keep you from feeling the symptoms of hypoglycemia, which may lead to severe hypoglycemia.
How can I prevent hypoglycemia if I have diabetes?
If you are taking insulin, a sulfonylurea, or a meglitinide, using your diabetes management plan and working with your health care team to adjust your plan as needed can help you prevent hypoglycemia. The following actions can also help prevent hypoglycemia:
Check blood glucose levels
Knowing your blood glucose level can help you decide how much medicine to take, what food to eat, and how physically active to be. To find out your blood glucose level, check yourself with a blood glucose meter as often as your doctor advises.
Hypoglycemia unawareness. Sometimes people with diabetes don’t feel or recognize the symptoms of hypoglycemia, a problem called hypoglycemia unawareness. If you have had hypoglycemia without feeling any symptoms, you may need to check your blood glucose more often so you know when you need to treat your hypoglycemia or take steps to prevent it. Be sure to check your blood glucose before you drive.
If you have hypoglycemia unawareness or have hypoglycemia often, ask your health care provider about a continuous glucose monitor (CGM). A CGM checks your blood glucose level at regular times throughout the day and night. CGMs can tell you if your blood glucose is falling quickly and sound an alarm if your blood glucose falls too low. CGM alarms can wake you up if you have hypoglycemia during sleep.
Eat regular meals and snacks
Your meal plan is key to preventing hypoglycemia. Eat regular meals and snacks with the correct amount of carbohydrates to help keep your blood glucose level from going too low. Also, if you drink alcoholic beverages, it’s best to eat some food at the same time.
Be physically active safely
Physical activity can lower your blood glucose during the activity and for hours afterward. To help prevent hypoglycemia, you may need to check your blood glucose before, during, and after physical activity and adjust your medicine or carbohydrate intake. For example, you might eat a snack before being physically active or decrease your insulin dose as directed by your health care provider to keep your blood glucose from dropping too low.
Work with your health care team
Tell your health care team if you have had hypoglycemia. Your health care team may adjust your diabetes medicines or other aspects of your management plan. Learn about balancing your medicines, eating plan, and physical activity to prevent hypoglycemia. Ask if you should have a glucagon emergency kit to carry with you at all times.
You can help prevent hypoglycemia by working with your health care team.
How do I treat hypoglycemia?
If you begin to feel one or more hypoglycemia symptoms, check your blood glucose. If your blood glucose level is below your target or less than 70, eat or drink 15 grams of carbohydrates right away. Examples include
1/2 cup (4 ounces) of fruit juice—not low-calorie or reduced sugar*
1/2 can (4 to 6 ounces) of soda—not low-calorie or reduced sugar
1 tablespoon of sugar, honey, or corn syrup
2 tablespoons of raisins
Wait 15 minutes and check your blood glucose again. If your glucose level is still low, eat or drink another 15 grams of glucose or carbohydrates. Check your blood glucose again after another 15 minutes. Repeat these steps until your glucose level is back to normal.
If your next meal is more than 1 hour away, have a snack to keep your blood glucose level in your target range. Try crackers or a piece of fruit.
*People who have kidney disease shouldn’t drink orange juice for their 15 grams of carbohydrates because it contains a lot of potassium. Apple, grape, or cranberry juice are good options.
If your blood glucose is below your target, take 15 grams of glucose or carbohydrates right away.
Treating hypoglycemia if you take acarbose or miglitol
If you take acarbose or miglitol along with diabetes medicines that can cause hypoglycemia, you will need to take glucose tablets or glucose gel if your blood glucose level is too low. Eating or drinking other sources of carbohydrates won’t raise your blood glucose level quickly enough.
What if I have severe hypoglycemia and can’t treat myself?
Someone will need to give you a glucagon injection if you have severe hypoglycemia. An injection of glucagon will quickly raise your blood glucose level. Talk with your health care provider about when and how to use a glucagon emergency kit. If you have an emergency kit, check the date on the package to make sure it hasn’t expired.
If you are likely to have severe hypoglycemia, teach your family, friends, and coworkers when and how to give you a glucagon injection. Also, tell your family, friends, and coworkers to call 911 right away after giving you a glucagon injection or if you don’t have a glucagon emergency kit with you.
If you have hypoglycemia often or have had severe hypoglycemia, you should wear a medical alert bracelet or pendant. A medical alert ID tells other people that you have diabetes and need care right away. Getting prompt care can help prevent the serious problems that hypoglycemia can cause.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank: Martha Funnell, M.S., R.N., C.D.E., University of Michigan Medical School
You can manage your diabetes and live a long and healthy life by taking care of yourself each day.
Diabetes can affect almost every part of your body. Therefore, you will need to manage your blood glucose levels, also called blood sugar. Managing your blood glucose, as well as your blood pressure and cholesterol, can help prevent the health problems that can occur when you have diabetes.
How can I manage my diabetes?
With the help of your health care team, you can create a diabetes self-care plan to manage your diabetes. Your self-care plan may include these steps:
Manage your diabetes ABCs
Knowing your diabetes ABCs will help you manage your blood glucose, blood pressure, and cholesterol. Stopping smoking if you smoke will also help you manage your diabetes. Working toward your ABC goals can help lower your chances of having a heart attack, stroke, or other diabetes problems.
A for the A1C test
The A1C test shows your average blood glucose level over the past 3 months. The A1C goal for many people with diabetes is below 7 percent. Ask your health care team what your goal should be.
B for Blood pressure
The blood pressure goal for most people with diabetes is below 140/90 mm Hg. Ask what your goal should be.
C for Cholesterol
You have two kinds of cholesterol in your blood: LDL and HDL. LDL or “bad” cholesterol can build up and clog your blood vessels. Too much bad cholesterol can cause a heart attack or stroke. HDL or “good” cholesterol helps remove the “bad” cholesterol from your blood vessels.
Ask your health care team what your cholesterol numbers should be. If you are over 40 years of age, you may need to take a statin drug for heart health.
S for Stop smoking
Not smoking is especially important for people with diabetes because both smoking and diabetes narrow blood vessels. Blood vessel narrowing makes your heart work harder. E-cigarettes aren’t a safe option either.
If you quit smoking
you will lower your risk for heart attack, stroke, nerve disease, kidney disease, diabetic eye disease, and amputation
your cholesterol and blood pressure levels may improve
your blood circulation will improve
you may have an easier time being physically active
If you smoke or use other tobacco products, stop. Ask for help so you don’t have to do it alone. You can start by calling the national quitline at 1-800-QUITNOW or 1-800-784-8669. For tips on quitting, go to SmokeFree.gov.
Keeping your A1C, blood pressure, and cholesterol levels close to your goals and stopping smoking may help prevent the long-term harmful effects of diabetes. These health problems include heart disease, stroke, kidney disease, nerve damage, and eye disease. You can keep track of your ABCs with a diabetes care record(PDF, 568 KB). Take it with you on your health care visits. Talk about your goals and how you are doing, and whether you need to make any changes in your diabetes care plan.
Follow your diabetes meal plan
Make a diabetes meal plan with help from your health care team. Following a meal plan will help you manage your blood glucose, blood pressure, and cholesterol.
Choose fruits and vegetables, beans, whole grains, chicken or turkey without the skin, fish, lean meats, and nonfat or low-fat milk and cheese. Drink water instead of sugar-sweetened beverages. Choose foods that are lower in calories, saturated fat, trans fat, sugar, and salt. Learn more about eating, diet, and nutrition with diabetes.
Make physical activity part of your daily routine
Set a goal to be more physically active. Try to work up to 30 minutes or more of physical activity on most days of the week.
Brisk walking and swimming are good ways to move more. If you are not active now, ask your health care team about the types and amounts of physical activity that are right for you. Learn more about being physically active with diabetes.
Swimming or water walking is a good way to move more.
Following your meal plan and being more active can help you stay at or get to a healthy weight. If you are overweight or obese, work with your health care team to create a weight-loss plan that is right for you.
Take your medicine
Take your medicines for diabetes and any other health problems, even when you feel good or have reached your blood glucose, blood pressure, and cholesterol goals. These medicines help you manage your ABCs. Ask your doctor if you need to take aspirin to prevent a heart attack or stroke. Tell your health care professional if you cannot afford your medicines or if you have any side effects from your medicines. Learn more about insulin and other diabetes medicines.
Check your blood glucose levels
For many people with diabetes, checking their blood glucose level each day is an important way to manage their diabetes. Monitoring your blood glucose level is most important if you take insulin. The results of blood glucose monitoring can help you make decisions about food, physical activity, and medicines.
Checking and recording your blood glucose level is an important part of managing diabetes.
The most common way to check your blood glucose level at home is with a blood glucose meter. You get a drop of blood by pricking the side of your fingertip with a lancet. Then you apply the blood to a test strip. The meter will show you how much glucose is in your blood at the moment.
Ask your health care team how often you should check your blood glucose levels. Make sure to keep a record of your blood glucose self-checks. You can print copies of this glucose self-check chart(PDF, 2 MB). Take these records with you when you visit your health care team.
What is continuous glucose monitoring?
Continuous glucose monitoring (CGM) is another way to check your glucose levels. Most CGM systems use a tiny sensor that you insert under your skin. The sensor measures glucose levels in the fluids between your body’s cells every few minutes and can show changes in your glucose level throughout the day and night. If the CGM system shows that your glucose is too high or too low, you should check your glucose with a blood glucose meter before making any changes to your eating plan, physical activity, or medicines. A CGM system is especially useful for people who use insulin and have problems with low blood glucose.
What are the recommended targets for blood glucose levels?
Many people with diabetes aim to keep their blood glucose at these normal levels:
Before a meal: 80 to 130 mg/dL
About 2 hours after a meal starts: less than 180 mg/dL
Talk with your health care team about the best target range for you. Be sure to tell your health care professional if your glucose levels often go above or below your target range.
What happens if my blood glucose level becomes too low?
Sometimes blood glucose levels drop below where they should be, which is called hypoglycemia. For most people with diabetes, the blood glucose level is too low when it is below 70 mg/dL.
What happens if my blood glucose level becomes too high?
Doctors call high blood glucose hyperglycemia.
Symptoms that your blood glucose levels may be too high include
feeling thirsty
feeling tired or weak
headaches
urinating often
blurred vision
If you often have high blood glucose levels or symptoms of high blood glucose, talk with your health care team. You may need a change in your diabetes meal plan, physical activity plan, or medicines.
Work with your health care team
Most people with diabetes get health care from a primary care professional. Primary care professionals include internists, family physicians, and pediatricians. Sometimes physician assistants and nurses with extra training, called nurse practitioners, provide primary care. You also will need to see other care professionals from time to time. A team of health care professionals can help you improve your diabetes self-care. Remember, you are the most important member of your health care team.
Besides a primary care professional, your health care team may include
When you see your doctor, review your diabetes self-care plan and blood glucose chart.
You should see your health care team at least twice a year, and more often if you are having problems or are having trouble reaching your blood glucose, blood pressure, or cholesterol goals. At each visit, be sure you have a blood pressure check, foot check, and weight check; and review your self-care plan. Talk with your health care team about your medicines and whether you need to adjust them. Routine health care will help you find and treat any health problems early, or may be able to help prevent them.
Feeling stressed, sad, or angry is common when you live with diabetes. Stress can raise your blood glucose levels, but you can learn ways to lower your stress. Try deep breathing, gardening, taking a walk, doing yoga, meditating, doing a hobby, or listening to your favorite music. Consider taking part in a diabetes education program or support group that teaches you techniques for managing stress. Learn more about healthy ways to cope with stress.
Depression is common among people with a chronic, or long-term, illness. Depression can get in the way of your efforts to manage your diabetes. Ask for help if you feel down. A mental health counselor, support group, clergy member, friend, or family member who will listen to your feelings may help you feel better.
Try to get 7 to 8 hours of sleep each night. Getting enough sleep can help improve your mood and energy level. You can take steps to improve your sleep habits. If you often feel sleepy during the day, you may have obstructive sleep apnea, a condition in which your breathing briefly stops many times during the night. Sleep apnea is common in people who have diabetes. Talk with your health care team if you think you have a sleep problem.
Remember, managing diabetes isn’t easy, but it’s worth it.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Pancreatic islets, also called islets of Langerhans, are tiny clusters of cells scattered throughout the pancreas. The pancreas is an organ about the size of a hand located behind the lower part of the stomach.
Pancreatic islets contain several types of cells, including beta cells, that produce the hormone insulin. The pancreas also makes enzymes that help the body digest and use food.
Pancreatic islets contain several types of cells, including beta cells, that produce the hormone insulin.
When the level of blood glucose, also called blood sugar, rises after a meal, the pancreas responds by releasing insulin into the bloodstream. Insulin helps cells throughout the body absorb glucose from the bloodstream and use it for energy.
Diabetes develops when the pancreas does not make enough insulin, the body's cells do not use insulin effectively, or both. As a result, glucose builds up in the blood instead of being absorbed by cells in the body.
In type 1 diabetes, the beta cells of the pancreas no longer make insulin because the body's immune system has attacked and destroyed them. The immune system protects people from infection by identifying and destroying bacteria, viruses, and other potentially harmful foreign substances. A person who has type 1 diabetes must take insulin daily to live. Type 2 diabetes usually begins with a condition called insulin resistance, in which the body has trouble using insulin effectively. Over time, insulin production declines as well, so many people with type 2 diabetes eventually need to take insulin.
What is pancreatic islet transplantation?
The two types of pancreatic islet transplantation are
allo-transplantation
auto-transplantation
Pancreatic islet allo-transplantation is a procedure in which islets from the pancreas of a deceased organ donor are purified, processed, and transferred into another person. Pancreatic islet allo-transplantation is currently labeled an experimental procedure until the transplantation technology is considered successful enough to be labeled therapeutic. For more information, see the section "What are the obstacles to pancreatic islet allo-transplantation?"
For each pancreatic islet allo-transplant infusion, researchers use specialized enzymes to remove islets from the pancreas of a single, deceased donor. The islets are purified and counted in a lab. Transplant patients typically receive two infusions with an average of 400,000 to 500,000 islets per infusion. Once implanted, the beta cells in these islets begin to make and release insulin.
Pancreatic islet allo-transplantation is performed in certain patients with type 1 diabetes whose blood glucose levels are difficult to control. The goals of the transplant are to help these patients achieve normal blood glucose levels with or without daily injections of insulin and to reduce or eliminate hypoglycemia unawareness—a dangerous condition in which a person with diabetes cannot feel the symptoms of hypoglycemia, or low blood glucose. When a person feels the symptoms of hypoglycemia, steps can be taken to bring blood glucose levels back to normal.
Pancreatic islet allo-transplants are only performed at hospitals that have received permission from the U.S. Food and Drug Administration (FDA) for clinical research on islet transplantation. The transplants are often performed by a radiologist—a doctor who specializes in medical imaging. The radiologist uses x rays and ultrasound to guide the placement of a thin, flexible tube called a catheter through a small incision in the upper abdomen—the area between the chest and hips—and into the portal vein of the liver. The portal vein is the major vein that supplies blood to the liver. The islets are then infused, or pushed, slowly into the liver through the catheter. Usually, the patient receives a local anesthetic and a sedative. In some cases, a surgeon performs the transplant using general anesthesia.
Patients often need two or more transplants to get enough functioning islets to stop or reduce their need for insulin injections.
Pancreatic islet allo-transplantation (above). In islet auto-transplantation, the islets are extracted from the patient's own pancreas.
Pancreatic islet auto-transplantation is performed following total pancreatectomy—the surgical removal of the whole pancreas—in patients with severe and chronic, or long lasting, pancreatitis that cannot be managed by other treatments. This procedure is not considered experimental. Patients with type 1 diabetes cannot receive pancreatic islet auto-transplantation. The procedure is performed in a hospital, and the patient receives general anesthesia. The surgeon first removes the pancreas and then extracts and purifies islets from the pancreas. Within hours, the islets are infused through a catheter into the patient's liver. The goal is to give the body enough healthy islets to make insulin.
What happens after pancreatic islet transplantation?
Pancreatic islets begin to release insulin soon after transplantation. However, full islet function and new blood vessel growth from the new islets take time. Transplant recipients usually take insulin injections until the islets are fully functional. They may also receive various medications before and after transplantation to promote successful implantation and long-term functioning of the islets. However, the autoimmune response that destroyed transplant recipients' own islets in the first place can happen again and attack the transplanted islets. Although the liver has been the traditional site for infusing the donor islets, researchers are investigating alternative sites, such as muscle tissue or another organ.
What are the benefits and risks of pancreatic islet allo-transplantation?
The benefits of pancreatic islet allo-transplantation include improved blood glucose control, reducing or eliminating the need for insulin injections to control diabetes, and preventing hypoglycemia. An alternative to islet transplantation is whole organ pancreas transplantation that is performed most often with kidney transplantation. The advantages of whole organ pancreas transplantation are less dependence on insulin and longer duration of organ function. The main disadvantage is that a whole organ transplant is a major surgery that involves a greater risk of complications and even death.
Pancreatic islet allo-transplantation can also help reverse hypoglycemia unawareness. Research has shown that even partial islet function after a transplant can eliminate hypoglycemia unawareness.
Improved blood glucose control from a successful allo-transplant may also slow or prevent the progression of diabetes problems, such as heart disease, kidney disease, and nerve or eye damage. Research to evaluate this possibility is ongoing.
The risks of pancreatic islet allo-transplantation include the risks associated with the transplant procedure—particularly bleeding and blood clots. The transplanted islets may not function well or may stop functioning entirely. Other risks are the side effects from the immunosuppressive medications that transplant recipients must take to stop the immune system from rejecting the transplanted islets. When a patient has received a kidney transplant and is already taking immunosuppressive medications, the only additional risks are the islet infusion and the side effects from the immunosuppressive medications given at the time of allo-transplantation. Immunosuppressive medications are not needed in the case of an auto-transplant because the infused cells come from the patient's own body. Read more in the section "What is the role of immunosuppressive medications?"
Collaborative Islet Transplant Registry Data
In its 2010 annual report,1 the Collaborative Islet Transplant Registry presented data on 571 patients who received pancreatic islet allo-transplants between 1999 and 2009. Although most procedures were pancreatic islet allo-transplants alone, 90 procedures were done in conjunction with a kidney transplant. The majority of the islet transplant patients received one or two infusions of islets; at the end of the decade, the average number of islets received per infusion was 463,000.
According to the report, about 60 percent of transplant recipients achieved insulin independence—defined as being able to stop insulin injections for at least 14 days—during the year following transplantation.
By the end of the second year, 50 percent of recipients were able to stop taking insulin for at least 14 days. However, long-term insulin independence is difficult to maintain, and eventually most recipients needed to start taking insulin again.
The report identified factors linked to better outcomes for recipients, including
age—35 years or older
lower pre-transplant triglyceride, or blood fat, levels
lower pre-transplant insulin use
The report noted that even partial function of the transplanted islets can improve blood glucose control and reduce the amount of insulin needed after loss of insulin independence.
What is the role of immunosuppressive medications?
Immunosuppressive medications are needed to prevent rejection—a common problem with any transplant.
Scientists have made many advances in islet transplantation in recent years. In 2000, islet transplantation researchers at the University of Alberta in Edmonton, Canada, reported their findings in the New England Journal of Medicine. Their transplant protocol, known as the Edmonton protocol, has since been adapted by transplant centers around the world and continues to be refined.
The Edmonton protocol introduced the use of a new combination of immunosuppressive medications, also called anti-rejection medications, including daclizumab (Zenapax), sirolimus (Rapamune), and tacrolimus (Prograf). Researchers continue to develop and study modifications to the Edmonton protocol, including improved medication regimens that promote successful transplants. Medication regimens vary from one transplant center to another. Examples of other immunosuppressive medications used in islet transplantation include antithymocyte globulin (Thymoglobulin), alemtuzumab (Campath), basiliximab (Simulect), belatacept (Nulojix), etanercept (Enbrel), everolimus (Zortress), and mycophenolate mofetil (CellCept, Myfortic). Researchers are also evaluating nonimmunosuppresive medications, such as exenatide (Byetta) and sitagliptin (Januvia).
Immunosuppressive medications have significant side effects, and their long-term effects are still not fully known. Immediate side effects may include mouth sores and gastrointestinal problems, such as upset stomach and diarrhea. Patients may also have
increased blood cholesterol, or blood fat, levels
high blood pressure
anemia, a condition in which red blood cells are fewer or smaller than normal, which prevents the body's cells from getting enough oxygen
fatigue
decreased white blood cell counts
decreased kidney function
increased susceptibility to bacterial and viral infections
Taking immunosuppressive medications also increases the risk of developing certain tumors and cancers.
Scientists are seeking ways to achieve immune tolerance of the transplanted islets, in which the patient's immune system no longer recognizes the islets as foreign. Immune tolerance would allow patients to maintain transplanted islets without long-term use of immunosuppressive medications. For example, one approach is to transplant islets encapsulated with a special coating, which may help to prevent rejection.
What are the obstacles to pancreatic islet allo-transplantation?
The shortage of islets from donors is a significant obstacle to widespread use of pancreatic islet allo-transplantation. According to the Organ Procurement and Transplantation Network, in 2011 there were about 8,000 deceased organ donors available in the United States.2 However, only 1,562 pancreases were recovered from donors in 2011.2 Also, many donated pancreases are not suitable for extracting islets for transplants because they do not meet the selection criteria, and islets are often damaged or destroyed during processing. Therefore, only a small number of islet transplants can be performed each year.
Researchers are pursuing various approaches to solve this shortage of islets, such as transplanting islets from a single, donated pancreas, using only a portion of the pancreas from a living donor, or using islets from pigs. Researchers have transplanted pig islets into other animals, including monkeys, by encapsulating the islets with a special coating or by using medications to prevent rejection. Another approach is creating islets from other types of cells, such as stem cells. New technologies could then be employed to grow islets in the lab.
Financial barriers also prevent the widespread use of islet allo-transplantation. Until the transplantation technology is considered successful enough to be labeled therapeutic rather than experimental, the costs of islet allo-transplants must be covered by research funds. Health insurance companies and Medicare generally do not cover experimental procedures. Federal law also does not allow health care providers or hospitals to charge patients or health insurance companies for research procedures. Some patient advocates and islet researchers feel that islet allo-transplantation is close to having a therapeutic label. The National Institutes of Health (NIH) currently supports studies that are working toward obtaining FDA licensure to reclassify islet allo-transplantation as therapeutic. In other countries, such as Canada and Scandinavia, islet allo-transplantation is no longer considered experimental and is an accepted therapy in certain patients.
A person who receives a pancreatic islet transplant should follow a meal plan worked out with a health care provider and dietitian. Immunosuppressive medications taken after the transplant can cause changes in a person's body, such as weight gain. A healthy diet after the transplant is important to control weight gain, blood pressure, blood cholesterol, and blood glucose levels.
Points to Remember
Pancreatic islets, also called islets of Langerhans, are tiny clusters of cells scattered throughout the pancreas. Pancreatic islets contain several types of cells, including beta cells, that produce the hormone insulin. Insulin helps cells throughout the body absorb glucose from the bloodstream and use it for energy.
Pancreatic islet allo-transplantation is a procedure in which islets from the pancreas of a deceased organ donor are purified, processed, and transferred into another person.
Pancreatic islet allo-transplantation is performed in certain patients with type 1 diabetes whose blood glucose levels are difficult to control. The goals of the transplant are to help these patients achieve normal blood glucose levels with or without daily injections of insulin and to reduce or eliminate hypoglycemia unawareness.
Pancreatic islet auto-transplantation is performed following total pancreatectomy in patients with severe and chronic pancreatitis that cannot be managed by other treatments. This procedure is not considered experimental. Patients with type 1 diabetes cannot receive pancreatic islet auto-transplantation.
The shortage of islets from donors is a significant obstacle to widespread use of pancreatic islet allo-transplantation. Financial barriers also prevent the widespread use of islet allo-transplantation. Until the transplantation technology is considered successful enough to be labeled therapeutic rather than experimental, the costs of islet allo-transplants must be covered by research funds.
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you? Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open? Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank: Marlon Levy, M.D., medical director of the Pancreas and Islet Cell Laboratory, Baylor University Medical Center and Baylor All Saints Medical Center
If you have diabetes and plan to have a baby, you should try to get your blood glucose levels close to your target range before you get pregnant.
Staying in your target range during pregnancy, which may be different than when you aren’t pregnant, is also important. High blood glucose, also called blood sugar, can harm your baby during the first weeks of pregnancy, even before you know you are pregnant. If you have diabetes and are already pregnant, see your doctor as soon as possible to make a plan to manage your diabetes. Working with your health care team and following your diabetes management plan can help you have a healthy pregnancy and a healthy baby.
Plan to manage your blood glucose before you get pregnant.
If you develop diabetes for the first time while you are pregnant, you have gestational diabetes.
How can diabetes affect my baby?
A baby’s organs, such as the brain, heart, kidneys, and lungs, start forming during the first 8 weeks of pregnancy. High blood glucose levels can be harmful during this early stage and can increase the chance that your baby will have birth defects, such as heart defects or defects of the brain or spine.
High blood glucose levels during pregnancy can also increase the chance that your baby will be born too early, weigh too much, or have breathing problems or low blood glucose right after birth.
High blood glucose also can increase the chance that you will have a miscarriage or a stillborn baby.1 Stillborn means the baby dies in the womb during the second half of pregnancy.
How can my diabetes affect me during pregnancy?
Hormonal and other changes in your body during pregnancy affect your blood glucose levels, so you might need to change how you manage your diabetes. Even if you’ve had diabetes for years, you may need to change your meal plan, physical activity routine, and medicines. If you have been taking an oral diabetes medicine, you may need to switch to insulin. As you get closer to your due date, your management plan might change again.
What health problems could I develop during pregnancy because of my diabetes?
Pregnancy can worsen certain long-term diabetes problems, such as eye problems and kidney disease, especially if your blood glucose levels are too high.
You also have a greater chance of developing preeclampsia, sometimes called toxemia, which is when you develop high blood pressure and too much protein in your urine during the second half of pregnancy. Preeclampsia can cause serious or life-threatening problems for you and your baby. The only cure for preeclampsia is to give birth. If you have preeclampsia and have reached 37 weeks of pregnancy, your doctor may want to deliver your baby early. Before 37 weeks, you and your doctor may consider other options to help your baby develop as much as possible before he or she is born.
How can I prepare for pregnancy if I have diabetes?
If you have diabetes, keeping your blood glucose as close to normal as possible before and during your pregnancy is important to stay healthy and have a healthy baby. Getting checkups before and during pregnancy, following your diabetes meal plan, being physically active as your health care team advises, and taking diabetes medicines if you need to will help you manage your diabetes. Stopping smoking and taking vitamins as your doctor advises also can help you and your baby stay healthy.
Work with your health care team
Regular visits with members of a health care team who are experts in diabetes and pregnancy will ensure that you and your baby get the best care. Your health care team may include
specialists who diagnose and treat diabetes-related problems, such as vision problems, kidney disease, and heart disease
a social worker or psychologist to help you cope with stress, worry, and the extra demands of pregnancy
You are the most important member of the team. Your health care team can give you expert advice, but you are the one who must manage your diabetes every day.
Talk with your health care team before you get pregnant.
Get a checkup
Have a complete checkup before you get pregnant or as soon as you know you are pregnant. Your doctor should check for
high blood pressure
eye disease
heart and blood vessel disease
nerve damage
kidney disease
thyroid disease
Pregnancy can make some diabetes health problems worse. To help prevent this, your health care team may recommend adjusting your treatment before you get pregnant.
Don’t smoke
Smoking can increase your chance of having a stillborn baby or a baby born too early.2 Smoking is especially harmful for people with diabetes. Smoking can increase diabetes-related health problems such as eye disease, heart disease, and kidney disease.
If you smoke or use other tobacco products, stop. Ask for help so you don’t have to do it alone. You can start by calling the national quitline at 1-800-QUITNOW or 1-800-784-8669. For tips on quitting, go to Smokefree.gov.
See a registered dietitian nutritionist
If you don’t already see a dietitian, you should start seeing one before you get pregnant. Your dietitian can help you learn what to eat, how much to eat, and when to eat to reach or stay at a healthy weight before you get pregnant. Together, you and your dietitian will create a meal plan to fit your needs, schedule, food preferences, medical conditions, medicines, and physical activity routine.
During pregnancy, some women need to make changes in their meal plan, such as adding extra calories, protein, and other nutrients. You will need to see your dietitian every few months during pregnancy as your dietary needs change.
Be physically active
Physical activity can help you reach your target blood glucose numbers. Being physically active can also help keep your blood pressure and cholesterol levels in a healthy range, relieve stress, strengthen your heart and bones, improve muscle strength, and keep your joints flexible.
Before getting pregnant, make physical activity a regular part of your life. Aim for 30 minutes of activity 5 days of the week.
Talk with your health care team about what activities are best for you during your pregnancy.
Physical activity can help you reach your target blood glucose numbers.
You should avoid drinking alcoholic beverages while you’re trying to get pregnant and throughout pregnancy. When you drink, the alcohol also affects your baby. Alcohol can lead to serious, lifelong health problems for your baby.
Adjust your medicines
Some medicines are not safe during pregnancy and you should stop taking them before you get pregnant. Tell your doctor about all the medicines you take, such as those for high cholesterol and high blood pressure. Your doctor can tell you which medicines to stop taking, and may prescribe a different medicine that is safe to use during pregnancy.
Doctors most often prescribe insulin for both type 1 and type 2 diabetes during pregnancy.3 If you’re already taking insulin, you might need to change the kind, the amount, or how and when you take it. You may need less insulin during your first trimester but probably will need more as you go through pregnancy. Your insulin needs may double or even triple as you get closer to your due date. Your health care team will work with you to create an insulin routine to meet your changing needs.
Take vitamin and mineral supplements
Folic acid is an important vitamin for you to take before and during pregnancy to protect your baby’s health. You’ll need to start taking folic acid at least 1 month before you get pregnant. You should take a multivitamin or supplement that contains at least 400 micrograms (mcg) of folic acid. Once you become pregnant, you should take 600 mcg daily.4 Ask your doctor if you should take other vitamins or minerals, such as iron or calcium supplements, or a multivitamin.
What do I need to know about blood glucose testing before and during pregnancy?
How often you check your blood glucose levels may change during pregnancy. You may need to check them more often than you do now. If you didn’t need to check your blood glucose before pregnancy, you will probably need to start. Ask your health care team how often and at what times you should check your blood glucose levels. Your blood glucose targets will change during pregnancy. Your health care team also may want you to check your ketone levels if your blood glucose is too high.
During your pregnancy, you may need to check your blood glucose levels more often.
Target blood glucose levels before pregnancy
When you’re planning to become pregnant, your daily blood glucose targets may be different than your previous targets. Ask your health care team which targets are right for you.
You can keep track of your blood glucose levels using My Daily Blood Glucose Record(PDF, 44 KB) . You can also use an electronic blood glucose tracking system on your computer or mobile device. Record the results every time you check your blood glucose. Your blood glucose records can help you and your health care team decide whether your diabetes care plan is working. You also can make notes about your insulin and ketones. Take your tracker with you when you visit your health care team.
Target blood glucose levels during pregnancy
Recommended daily target blood glucose numbers for most pregnant women with diabetes are
Before meals, at bedtime, and overnight: 90 or less
1 hour after eating: 130 to 140 or less
2 hours after eating: 120 or less3
Ask your doctor what targets are right for you. If you have type 1 diabetes, your targets may be higher so you don’t develop low blood glucose, also called hypoglycemia.
A1C numbers
Another way to see whether you’re meeting your targets is to have an A1C blood test. Results of the A1C test reflect your average blood glucose levels during the past 3 months. Most women with diabetes should aim for an A1C as close to normal as possible—ideally below 6.5 percent—before getting pregnant.3 After the first 3 months of pregnancy, your target may be as low as 6 percent.3 These targets may be different than A1C goals you’ve had in the past. Your doctor can help you set A1C targets that are best for you.
Ketone levels
When your blood glucose is too high or if you’re not eating enough, your body might make ketones. Ketones in your urine or blood mean your body is using fat for energy instead of glucose. Burning large amounts of fat instead of glucose can be harmful to your health and your baby’s health.
You can prevent serious health problems by checking for ketones. Your doctor might recommend you test your urine or blood daily for ketones or when your blood glucose is above a certain level, such as 200. If you use an insulin pump, your doctor might advise you to test for ketones when your blood glucose level is higher than expected. Your health care team can teach you how and when to test your urine or blood for ketones.
Talk with your doctor about what to do if you have ketones. Your doctor might suggest making changes in the amount of insulin you take or when you take it. Your doctor also may recommend a change in meals or snacks if you need to consume more carbohydrates.
What tests will check my baby’s health during pregnancy?
You will have tests throughout your pregnancy, such as blood tests and ultrasounds, to check your baby’s health. Talk with your health care team about what prenatal tests you’ll have and when you might have them.
References
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank: Boyd E. Metzger, MD, Northwestern University Feinberg School of Medicine
Perhaps you have learned that you have a high chance of developing type 2 diabetes, the most common type of diabetes. You might be overweight or have a parent, brother, or sister with type 2 diabetes. Maybe you had gestational diabetes, which is diabetes that develops during pregnancy. These are just a few examples of factors that can raise your chances of developing type 2 diabetes.
Diabetes can cause serious health problems, such as heart disease, stroke, and eye and foot problems. Prediabetes also can cause health problems. The good news is that type 2 diabetes can be delayed or even prevented. The longer you have diabetes, the more likely you are to develop health problems, so delaying diabetes by even a few years will benefit your health. You can help prevent or delay type 2 diabetes by losing a modest amount of weight by following a reduced-calorie eating plan and being physically active most days of the week. Ask your doctor if you should take the diabetes drug metformin to help prevent or delay type 2 diabetes.1
How can I lower my chances of developing type 2 diabetes?
Research such as the Diabetes Prevention Program shows that you can do a lot to reduce your chances of developing type 2 diabetes. Here are some things you can change to lower your risk:
Lose weight and keep it off. You may be able to prevent or delay diabetes by losing 5 to 7 percent of your starting weight.1 For instance, if you weigh 200 pounds, your goal would be to lose about 10 to 14 pounds.
Move more. Get at least 30 minutes of physical activity 5 days a week. If you have not been active, talk with your health care professional about which activities are best. Start slowly to build up to your goal.
Eat healthy foods most of the time. Eat smaller portions to reduce the amount of calories you eat each day and help you lose weight. Choosing foods with less fat is another way to reduce calories. Drink water instead of sweetened beverages.
Ask your health care professional about what other changes you can make to prevent or delay type 2 diabetes.
Most often, your best chance for preventing type 2 diabetes is to make lifestyle changes that work for you long term. Get started with Your Game Plan to Prevent Type 2 Diabetes.
Losing weight through healthy eating and regular physical activity can help you prevent type 2 diabetes.
What should I do if my health care professional told me I have prediabetes?
Prediabetes is when your blood glucose, also called blood sugar, levels are higher than normal, but not high enough to be called diabetes. Having prediabetes is serious because it raises your chance of developing type 2 diabetes. Many of the same factors that raise your chance of developing type 2 diabetes put you at risk for prediabetes.
Other names for prediabetes include impaired fasting glucose or impaired glucose tolerance. Some people call prediabetes “borderline diabetes.”
About 1 in 3 Americans has prediabetes, according to recent diabetes statistics from the Centers for Disease Control and Prevention. You won’t know if you have prediabetes unless you are tested.
If you have prediabetes, you can lower your chance of developing type 2 diabetes. Lose weight if you need to, become more physically active, and follow a reduced-calorie eating plan.
Being physically active is one way to help prevent prediabetes from progressing to type 2 diabetes.
If I had gestational diabetes when I was pregnant, how can I lower my chances of developing type 2 diabetes?
Gestational diabetes is a type of diabetes that develops during pregnancy. Most of the time, gestational diabetes goes away after your baby is born. Even if your gestational diabetes goes away, you still have a greater chance of developing type 2 diabetes within 5 to 10 years. Your child may also be more likely to become obese and develop type 2 diabetes later in life. Making healthy choices helps the whole family and may protect your child from becoming obese or developing diabetes.
Being physically active together is a great way to lower your own and your child’s chance of developing type 2 diabetes.
Here are steps you should take for yourself and your child if you had gestational diabetes:
Get tested for diabetes 6 to 12 weeks after your baby is born. If your blood glucose is still high, you may have type 2 diabetes. If your blood glucose is normal, you should get tested every 3 years to see if you have developed type 2 diabetes.
Be more active and make healthy food choices to get back to a healthy weight.
Breastfeed your baby. Breastfeeding gives your baby the right balance of nutrients and helps you burn calories.
Ask your doctor if you should take the diabetes drug metformin to help prevent type 2 diabetes.1
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Your chances of developing type 2 diabetes depend on a combination of risk factors such as your genes and lifestyle. Although you can’t change risk factors such as family history, age, or ethnicity, you can change lifestyle risk factors around eating, physical activity, and weight. These lifestyle changes can affect your chances of developing type 2 diabetes.
Read about risk factors for type 2 diabetes below and see which ones apply to you. Taking action on the factors you can change can help you delay or prevent type 2 diabetes.
You are more likely to develop type 2 diabetes if you
have acanthosis nigricans—dark, thick, and velvety skin around your neck or armpits
You can also take the Diabetes Risk Test to learn about your risk for type 2 diabetes.
To see if your weight puts you at risk for type 2 diabetes, find your height in the Body Mass Index (BMI) charts below. If your weight is equal to or more than the weight listed, you have a greater chance of developing the disease.
If you are not Asian American or Pacific Islander
If you are Asian American
If you are Pacific Islander
At-risk BMI = 25
At-risk BMI = 23
At-risk BMI = 26
Height
Weight
Height
Weight
Height
Weight
4'10"
119
4'10"
110
4'10"
124
4'11"
124
4'11"
114
4'11"
128
5'0"
128
5'0"
118
5'0"
133
5'1"
132
5'1"
122
5'1"
137
5'2"
136
5'2"
126
5'2"
142
5'3"
141
5'3"
130
5'3"
146
5'4"
145
5'4"
134
5'4"
151
5'5"
150
5'5"
138
5'5"
156
5'6"
155
5'6"
142
5'6"
161
5'7"
159
5'7"
146
5'7"
166
5'8"
164
5'8"
151
5'8"
171
5'9"
169
5'9"
155
5'9"
176
5'10"
174
5'10"
160
5'10"
181
5'11"
179
5'11"
165
5'11"
186
6'0"
184
6'0"
169
6'0"
191
6'1"
189
6'1"
174
6'1"
197
6'2"
194
6'2"
179
6'2"
202
6'3"
200
6'3"
184
6'3"
208
6'4"
205
6'4"
189
6'4"
213
What can I do to prevent type 2 diabetes?
You can take steps to help prevent or delay type 2 diabetes by losing weight if you are overweight, eating fewer calories, and being more physically active. Talk with your health care professional about any of the health conditions listed above that may require medical treatment. Managing these health problems may help reduce your chances of developing type 2 diabetes. Also, ask your health care professional about any medicines you take that might increase your risk.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Symptoms of type 1 diabetes can start quickly, in a matter of weeks. Symptoms of type 2 diabetes often develop slowly—over the course of several years—and can be so mild that you might not even notice them. Many people with type 2 diabetes have no symptoms. Some people do not find out they have the disease until they have diabetes-related health problems, such as blurred vision or heart trouble.
What causes type 1 diabetes?
Type 1 diabetes occurs when your immune system, the body’s system for fighting infection, attacks and destroys the insulin-producing beta cells of the pancreas. Scientists think type 1 diabetes is caused by genes and environmental factors, such as viruses, that might trigger the disease. Studies such as TrialNet are working to pinpoint causes of type 1 diabetes and possible ways to prevent or slow the disease.
What causes type 2 diabetes?
Type 2 diabetes—the most common form of diabetes—is caused by several factors, including lifestyle factors and genes.
Overweight, obesity, and physical inactivity
You are more likely to develop type 2 diabetes if you are not physically active and are overweight or obese. Extra weight sometimes causes insulin resistance and is common in people with type 2 diabetes. The location of body fat also makes a difference. Extra belly fat is linked to insulin resistance, type 2 diabetes, and heart and blood vessel disease. To see if your weight puts you at risk for type 2 diabetes, check out these Body Mass Index (BMI) charts.
Insulin resistance
Type 2 diabetes usually begins with insulin resistance, a condition in which muscle, liver, and fat cells do not use insulin well. As a result, your body needs more insulin to help glucose enter cells. At first, the pancreas makes more insulin to keep up with the added demand. Over time, the pancreas can’t make enough insulin, and blood glucose levels rise.
Genes and family history
As in type 1 diabetes, certain genes may make you more likely to develop type 2 diabetes. The disease tends to run in families and occurs more often in these racial/ethnic groups:
African Americans
Alaska Natives
American Indians
Asian Americans
Hispanics/Latinos
Native Hawaiians
Pacific Islanders
Genes also can increase the risk of type 2 diabetes by increasing a person’s tendency to become overweight or obese.
What causes gestational diabetes?
Scientists believe gestational diabetes, a type of diabetes that develops during pregnancy, is caused by the hormonal changes of pregnancy along with genetic and lifestyle factors.
Insulin resistance
Hormones produced by the placenta contribute to insulin resistance, which occurs in all women during late pregnancy. Most pregnant women can produce enough insulin to overcome insulin resistance, but some cannot. Gestational diabetes occurs when the pancreas can’t make enough insulin.
As with type 2 diabetes, extra weight is linked to gestational diabetes. Women who are overweight or obese may already have insulin resistance when they become pregnant. Gaining too much weight during pregnancy may also be a factor.
Hormonal changes, extra weight, and family history can contribute to gestational diabetes.
Genes and family history
Having a family history of diabetes makes it more likely that a woman will develop gestational diabetes, which suggests that genes play a role. Genes may also explain why the disorder occurs more often in African Americans, American Indians, Asians, and Hispanics/Latinas.
What else can cause diabetes?
Genetic mutations, other diseases, damage to the pancreas, and certain medicines may also cause diabetes.
Genetic mutations
Monogenic diabetes is caused by mutations, or changes, in a single gene. These changes are usually passed through families, but sometimes the gene mutation happens on its own. Most of these gene mutations cause diabetes by making the pancreas less able to make insulin. The most common types of monogenic diabetes are neonatal diabetes and maturity-onset diabetes of the young (MODY). Neonatal diabetes occurs in the first 6 months of life. Doctors usually diagnose MODY during adolescence or early adulthood, but sometimes the disease is not diagnosed until later in life.
Cystic fibrosis produces thick mucus that causes scarring in the pancreas. This scarring can prevent the pancreas from making enough insulin.
Hemochromatosis causes the body to store too much iron. If the disease is not treated, iron can build up in and damage the pancreas and other organs.
Hormonal diseases
Some hormonal diseases cause the body to produce too much of certain hormones, which sometimes cause insulin resistance and diabetes.
Acromegaly occurs when the body produces too much growth hormone.
Hyperthyroidism occurs when the thyroid gland produces too much thyroid hormone.
Damage to or removal of the pancreas
Pancreatitis, pancreatic cancer, and trauma can all harm the beta cells or make them less able to produce insulin, resulting in diabetes. If the damaged pancreas is removed, diabetes will occur due to the loss of the beta cells.
Medicines
Sometimes certain medicines can harm beta cells or disrupt the way insulin works. These include
niacin, a type of vitamin B3
certain types of diuretics, also called water pills
anti-rejection medicines, used to help stop the body from rejecting a transplanted organ
Statins, which are medicines to reduce LDL (“bad”) cholesterol levels, can slightly increase the chance that you’ll develop diabetes. However, statins help protect you from heart disease and stroke. For this reason, the strong benefits of taking statins outweigh the small chance that you could develop diabetes.
If you take any of these medicines and are concerned about their side effects, talk with your doctor.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Take Care of Your Diabetes During Sick Days & Special Times
Diabetes is part of your life. You can learn how to take care of yourself and your diabetes when you’re sick, when you’re at school or work, when you’re away from home, when an emergency or a natural disaster happens, or when you’re thinking about having a baby or are pregnant.
When You’re Sick
Having a cold, the flu, or an infection can raise your blood glucose levels. Being sick puts stress on your body. Your body releases hormones to deal with the stress and to fight the sickness. Higher hormone levels can also cause high blood glucose levels. You should have a plan for managing your diabetes when you’re sick. The first step is to talk with your health care team and write down
how often to check your blood glucose levels
whether you should check for ketones in your blood or urine
whether you should change your usual dose of your diabetes medicines
what to eat and drink
when to call your doctor
People who are sick sometimes feel as though they can’t eat as much or can’t keep food down, which can cause low blood glucose levels. Consuming carbohydrate-rich drinks or snacks can help prevent low blood glucose.
If you are sick, your health care team may recommend the following:
Check your blood glucose levels at least four times a day and write down the results in your record book. Keep your results handy so you can report the results to your health care team.
Keep taking your diabetes medicines, even if you can’t eat.
Drink at least 1 cup, or 8 ounces, of water or other calorie-free, caffeine-free liquid every hour while you’re awake.
If you can’t eat your usual food, try eating or drinking any of the following to prevent low blood glucose levels:
juice
saltine crackers
dry toast
soup
broth or bouillon
ice pops or sherbet
gelatin that isn’t sugar-free
milk
yogurt
soda that isn’t sugar-free
Your doctor may ask that you call right away if
your blood glucose levels are above 240 even though you’ve taken your diabetes medicines
your urine or blood ketone levels are above normal
you vomit more than once
you have diarrhea for more than 6 hours
you have trouble breathing
you have a high fever
you can’t think clearly or you feel more drowsy than usual
You should call your doctor if you have questions about taking care of yourself.
When You’re at School or Work
Take care of your diabetes when you’re at school or at work:
Follow your healthy eating plan.
Take your medicines and check your blood glucose levels as usual.
Tell your teachers, friends, or close coworkers that you have diabetes and teach them about the signs of low blood glucose. You may need their help if your blood glucose levels drop too low.
Keep snacks nearby and carry some with you at all times to treat low blood glucose.
If you have trained diabetes staff at your school or work, tell them that you have diabetes.
Wear or carry an identification tag or card that says you have diabetes.
Tell your teachers, friends, or close coworkers about the signs of low blood glucose. You may need their help if your blood glucose levels drop too low.
When You’re Away from Home
These tips can help you when you’re away from home:
Get all your vaccines and immunizations, or shots, before you travel. Find out what shot you need for where you’re going, and make sure you get the right shots on time.
Follow your healthy eating plan as much as possible when you eat out. Always carry a snack with you in case you have to wait for a waiter to serve you.
Limit alcoholic beverages. Ask your health care team how many alcoholic beverages you can safely drink. Eat something when you drink to prevent low blood glucose.
If you’re taking a long trip by car, check your blood glucose levels before driving. Stop and check your blood glucose levels every 2 hours.
Always carry your diabetes medicines and supplies in the car where you can reach them in case your blood glucose levels drop too low.
In case you can’t leave for home on time, bring twice the amount of diabetes supplies and medicines you normally need.
Take comfortable, well-fitting shoes on vacation. You’ll probably be walking more than usual. Keep your medical insurance card, emergency phone numbers, and a first aid kit handy.
Wear or carry an identification tag or card that says you have diabetes.
If you’re going to be away for a long time, ask your doctor for a written prescription for your diabetes medicines and the name of a doctor in the place you’re going to visit.
Don’t count on buying extra supplies when you’re traveling, especially if you’re going to another country. Different countries use different kinds of diabetes medicines.
When You’re Flying on a Plane
These tips can help you when you’re flying on a plane:
Ask your health care team in advance how to adjust your medicines, especially your insulin, if you’re traveling across time zones.
Take a letter from your doctor stating you have diabetes. The letter should include a list of all the medical supplies and medicines you need on the plane. In the letter, the doctor should also include a list of any devices that shouldn’t go through an x-ray machine.
Carry your diabetes medicines and your blood testing supplies with you on the plane. Never put these items in your checked baggage.
Bring food for meals and snacks on the plane.
If you use an insulin pump, ask airport security to check the device by hand. X-ray machines can damage insulin pumps, whether the pump is on your body or in your luggage.
When on a plane, get up from your seat and walk around when possible.
Read more about planning for travel and travel safety if you have diabetes in Have Diabetes. Will Travel(319 KB).
Bring food for meals and snacks on the plane.
When an Emergency or a Natural Disaster Happens
Everyone with diabetes should be prepared for emergencies and natural disasters, such as power outages or hurricanes. Always have a disaster kit ready. Include everything you need to take care of your diabetes, such as
a blood glucose meter, lancets, and testing strips
your diabetes medicines
insulin, syringes, and an insulated bag to keep insulin cool, if you take insulin
a glucagon kit if you take insulin or if recommended by your doctor
glucose tablets and other food or drinks to treat low blood glucose
antibiotic cream or ointment
a copy of your medical information, including a list of your conditions, medicines, and recent lab test results
a list of your prescription names with dosage information and prescription numbers from your pharmacy
phone numbers for the American Red Cross and other disaster relief groups
You also might want to include some food that doesn’t spoil, such as canned or dried food, along with bottled water. Read more about preparing for an emergency at the Centers for Disease Control and Prevention Emergency Preparedness and You website at www.emergency.cdc.gov/preparedness.
If You’re a Woman and Planning a Pregnancy
Keeping your blood glucose levels near normal before and during pregnancy helps protect both you and your baby. Even before you become pregnant, your blood glucose levels should be close to the normal range.
Your health care team can work with you to get your blood glucose levels under control before you try to get pregnant. If you’re already pregnant and you have diabetes, see your doctor right away. You can take steps to bring your blood glucose levels close to normal.
Your insulin needs may change when you’re pregnant. Your doctor may want you to take more insulin and check your blood glucose levels more often.
If you plan to have a baby,
work with your health care team to get your blood glucose levels as close to the normal range as possible
see a doctor who has experience taking care of pregnant women with diabetes
don’t smoke, drink alcoholic beverages, or use harmful drugs
follow your healthy eating plan
Be sure to have your eyes, heart and blood vessels, blood pressure, and kidneys checked. Your doctor should also check for nerve damage. Pregnancy can make some health problems worse.
More information about diabetes and pregnancy is provided in the NIDDK health topic, Diabetes and Pregnancy.
Your health care team can work with you to get your blood glucose levels under control before you try to get pregnant. If you’re already pregnant, see your doctor right away.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK would like to thank:
Michael L. Parchman, M.D., M.P.H., F.A.A.F.P., MacColl Center for Health Care Innovation, Group Health Research Institute; Marion J. Franz, M.S., R.D., L.D., C.D.E., Minneapolis, Minnesota
Taking Care of Your Diabetes Means Taking Care of Your Heart
Diabetes and Heart Disease
For people with diabetes, heart disease can be a serious health problem. Many people don’t know that having diabetes means that you have a greater chance of having heart problems such as a heart attack or stroke. Taking care of your diabetes can also help you take care of your heart. Use the tools in this tip sheet to help. They are:
A list of things you can do such as eating healthy foods and getting more active.
A form to write down and track your A1C, blood pressure, and cholesterol numbers.
What can I do to lower my chances of getting heart disease?
What should my goals be for A1C, blood pressure, and cholesterol?
What can I do to reach these goals?
Should I take medicine that can protect my heart such as aspirin or a statin?
Eat well.
Eat foods that are high in fiber such as whole grain breads and cereals, brown rice, lentils, beans, fruits, and vegetables.
Eat foods with heart-healthy fats such as fish, nuts, seeds, and avocado.
Eat foods low in saturated and transfats such as lean meat, chicken without the skin, fish, and non-fat or low-fat milk, yogurt, and cheese.
Use oils when cooking food instead of butter, cream, shortening, lard, or stick margarine.
Limit desserts such as cookies and ice cream to only 1 or 2 times a week.
Eat smaller amounts of foods that are high in fat, sugar, or salt. For example, if you want french fries, order the kid-sized portion.
Bake, broil, or grill food instead of frying.
Do not add salt to food.
Stop smoking.
Ask for help or call 1-800-784-8669 (1-800-QUIT-NOW).
Be active.
Be active for 30 minutes or more each day. It’s okay to be active for 10 minutes at a time, 3 times a day.
Walk, dance, swim, or ride a bike.
Take your medicine.
Take medicines the way your doctor or health care team tells you to.
Do not stop taking your medicines until you talk to your doctor.
Ask your pharmacist or doctor any questions you have about your medicines.
Cope with stress as best you can.
Ask for help if you feel down. Talk to a mental health counselor, member of the clergy, friend, or family member who will listen to your concerns.
Tell your family members and friends how they can best help and support you.
Your Diabetes Record Form
Use this form to keep track of your A1C, blood pressure, and cholesterol numbers. These terms are explained below the Diabetes Record Form.
Write down the date and results for each test or blood pressure check you get.
Take this form with you on your health care visits. Show it to your health care team.
Talk about your goals and how you are doing.
Diabetes Record Form
A1C
At each visit:
My Goal
Date
Result
Blood Pressure (BP)
At each visit:
My Goal
Date
Result
Cholesterol
At each visit:
My Goal
Date
Result
A1C test (A-one-C)
What is it?
The A1C is a blood test that measures your average blood sugar (glucose) level over the past three months. It is different from the blood sugar checks you do each day.
Why is it important?
You need to know your blood sugar levels over time. You don’t want those numbers to get too high. High levels of blood sugar can harm your heart, blood vessels, kidneys, feet, and eyes.
What is the A1C goal?
The A1C goal for many people with diabetes is below 7. It may be different if you are an older adult (over 65), have had diabetes for a long time, or your blood sugar often gets too low. Ask what your goal should be.
Blood Pressure
What is it?
Blood pressure is the force of your blood against the walls of your blood vessels.
Why is it important?
If your blood pressure gets too high, it makes your heart work too hard. It can cause a heart attack, stroke, and damage your kidneys and eyes.
What is the blood pressure goal?
The blood pressure goal for most people with diabetes is below 140/90. It may be different for you. Ask what your goal should be.
Cholesterol
What is it?
There are two kinds of cholesterol in your blood: LDL and HDL.
Why is it important?
LDL or “bad” cholesterol can build up and clog your blood vessels. It can cause a heart attack or stroke. HDL or “good” cholesterol helps remove the “bad” cholesterol from your blood vessels.
What are the LDL and HDL goals?
These goals are different for different people. Ask what your cholesterol numbers should be. If you are over 40 years of age, you may need to take medicine such as a statin to lower your cholesterol and protect your heart.
The U.S. Department of Health and Human Services’ National Diabetes Education Program (NDEP) is jointly sponsored by the National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC) with the support of more than 200 partner organizations.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The A1C test is a blood test that provides information about a person’s average levels of blood glucose, also called blood sugar, over the past 3 months. The A1C test is sometimes called the hemoglobin A1c, HbA1c, or glycohemoglobin test. The A1C test is the primary test used for diabetes management and diabetes research.
How does the A1C test work?
The A1C test is based on the attachment of glucose to hemoglobin, the protein in red blood cells that carries oxygen. In the body, red blood cells are constantly forming and dying, but typically they live for about 3 months. Thus, the A1C test reflects the average of a person’s blood glucose levels over the past 3 months. The A1C test result is reported as a percentage. The higher the percentage, the higher a person’s blood glucose levels have been. A normal A1C level is below 5.7 percent.
Can the A1C test be used to diagnose type 2 diabetes and prediabetes?
Yes. In 2009, an international expert committee recommended the A1C test as one of the tests available to help diagnose type 2 diabetes and prediabetes.1 Previously, only the traditional blood glucose tests were used to diagnose diabetes and prediabetes.
Because the A1C test does not require fasting and blood can be drawn for the test at any time of day, experts are hoping its convenience will allow more people to get tested—thus, decreasing the number of people with undiagnosed diabetes. However, some medical organizations continue to recommend using blood glucose tests for diagnosis.
Why should a person be tested for diabetes?
Testing is especially important because early in the disease diabetes has no symptoms. Although no test is perfect, the A1C and blood glucose tests are the best tools available to diagnose diabetes—a serious and lifelong disease.
Testing enables health care providers to find and treat diabetes before complications occur and to find and treat prediabetes, which can delay or prevent type 2 diabetes from developing.
Has the A1C test improved?
Yes. A1C laboratory tests are now standardized. In the past, the A1C test was not recommended for diagnosis of type 2 diabetes and prediabetes because the many different types of A1C tests could give varied results. The accuracy has been improved by the National Glycohemoglobin Standardization Program (NGSP), which developed standards for the A1C tests.
The NGSP certifies that manufacturers of A1C tests provide tests that are consistent with those used in a major diabetes study. The study established current A1C goals for blood glucose control that can reduce the occurrence of diabetes complications, such as blindness and blood vessel disease.2
How is the A1C test used to diagnose type 2 diabetes and prediabetes?
The A1C test can be used to diagnose type 2 diabetes and prediabetes alone or in combination with other diabetes tests. When the A1C test is used for diagnosis, the blood sample must be sent to a laboratory that uses an NGSP-certified method for analysis to ensure the results are standardized.
Blood samples analyzed in a health care provider’s office, known as point-of-care (POC) tests, are not standardized for diagnosing diabetes. The following table provides the percentages that indicate diagnoses of normal, diabetes, and prediabetes according to A1C levels.
*Any test for diagnosis of diabetes requires confirmation with a second measurement unless there are clear symptoms of diabetes.
Diagnosis*
A1C Level
Normal
below 5.7 percent
Diabetes
6.5 percent or above
Prediabetes
5.7 to 6.4 percent
Having prediabetes is a risk factor for getting type 2 diabetes. People with prediabetes may be retested each year. Within the prediabetes A1C range of 5.7 to 6.4 percent, the higher the A1C, the greater the risk of diabetes. Those with prediabetes are likely to develop type 2 diabetes within 10 years, but they can take steps to prevent or delay diabetes.
Is the A1C test used during pregnancy?
The A1C test may be used at the first visit to the health care provider during pregnancy to see if women with risk factors had undiagnosed diabetes before becoming pregnant. After that, the oral glucose tolerance test (OGTT) is used to test for diabetes that develops during pregnancy—known as gestational diabetes. After delivery, women who had gestational diabetes should be tested for persistent diabetes. Blood glucose tests, rather than the A1C test, should be used for testing within 12 weeks of delivery.
Can blood glucose tests still be used for diagnosing type 2 diabetes and prediabetes?
Yes. The standard blood glucose tests used for diagnosing type 2 diabetes and prediabetes-the fasting plasma glucose (FPG) test and the OGTT—are still recommended. The random plasma glucose test, also called the casual glucose test, may be used for diagnosing diabetes when symptoms of diabetes are present. In some cases, the A1C test is used to help health care providers confirm the results of a blood glucose test.
Can the A1C test result in a different diagnosis than the blood glucose tests?
Yes. In some people, a blood glucose test may indicate a diagnosis of diabetes while an A1C test does not. The reverse can also occur—an A1C test may indicate a diagnosis of diabetes even though a blood glucose test does not. Because of these variations in test results, health care providers repeat tests before making a diagnosis.
People with differing test results may be in an early stage of the disease, where blood glucose levels have not risen high enough to show on every test. Sometimes, making simple changes in lifestyle—losing a small amount of weight and increasing physical activity—can help people in this early stage reverse diabetes or delay its onset.
More information about diagnosing diabetes and prediabetes is provided in the NIDDK health topic, Diagnosis of Diabetes and Prediabetes, or by calling 1–800–860–8747.
Are diabetes blood test results always accurate?
All laboratory test results can vary from day to day and from test to test. Results can vary
within the person being tested. A person’s blood glucose levels normally move up and down depending on meals, exercise, sickness, and stress.
between different tests. Each test measures blood glucose levels in a different way. For example, the FPG test measures glucose that is floating free in the blood after fasting and only shows the blood glucose level at the time of the test. Repeated blood glucose tests, such as self-monitoring several times a day with a home meter, can record the natural variations of blood glucose levels during the day. The A1C test represents the amount of glucose attached to hemoglobin, so it reflects an average of all the blood glucose levels a person may experience over 3 months. The A1C test will not show day-to-day changes.
The following chart shows how multiple blood glucose measurements over 4 days compare with an A1C measurement.
Blood Glucose Measurements Compared with A1C Measurements Over 4 Days
Note: Blood glucose (mg/dL) measurements were taken four times per day (fasting or pre-breakfast, pre-lunch, pre-dinner, and bedtime).
The straight black line indicates an A1C measurement of 7.0 percent. The blue line shows blood glucose test results from self-monitoring four times a day over a 4-day period.
within the same test. Even when the same blood sample is repeatedly measured in the same laboratory, the results may vary due to small changes in temperature, equipment, or sample handling.
Health care providers take these variations into account when considering test results and repeat laboratory tests for confirmation. Diabetes develops over time, so even with variations in test results, health care providers can tell when overall blood glucose levels are becoming too high.
Comparing test results from different laboratories can be misleading. People should consider requesting new laboratory tests when they change health care providers, or if their health care provider’s office changes the laboratory or clinic it uses for blood testing.
How accurate is the A1C test?
The A1C test result can be up to 0.5 percent higher or lower than the actual percentage. This means an A1C measured as 7.0 percent could indicate a true A1C anywhere in the range from ~6.5 to 7.5 percent. Health care providers can visit www.ngsp.org to find information about the accuracy of the A1C test used by their laboratory.
The drawing below illustrates the range of possible true values when an A1C is 7.0 percent on the lab report. This range is based on the inherent variability of the laboratory test, often referred to as the coefficient of variation. Different degrees of laboratory variability result in different ranges of possible true values. The range illustrated is the maximum allowed by test methods approved by NGSP.
Courtesy of David Aron, M.D., Louis Stokes Department of Veterans Affairs Medical Center
To put the A1C test into perspective, an FPG test result of 126 mg/dL obtained from a laboratory test accounting for typical variability within an individual person could indicate a true FPG anywhere in the range from ~110 to 142 mg/dL. This variation will be even greater if the blood sample is not processed promptly or is not put on ice, causing blood glucose levels in the sample to decrease. The drawing below illustrates the range of possible true values for an FPG of 126 mg/dL.
Courtesy of David Aron, M.D., Louis Stokes Department of Veterans Affairs Medical Center
Can the A1C test give false results?
Yes, for some people. The A1C test can be unreliable for diagnosing or monitoring diabetes in people with certain conditions that are known to interfere with the results. Interference should be suspected when A1C results seem very different from the results of a blood glucose test.
People of African, Mediterranean, or Southeast Asian descent, or people with family members with sickle cell anemia or a thalassemia are particularly at risk of interference. People in these groups may have a less common type of hemoglobin, known as a hemoglobin variant, that can interfere with some A1C tests. Most people with a hemoglobin variant have no symptoms and may not know that they carry this type of hemoglobin.
Not all of the A1C tests are unreliable for people with a hemoglobin variant. People with false results from one type of A1C test may need a different type of A1C test for measuring their average blood glucose level. The NGSP provides information for health care providers about which A1C tests are appropriate to use for specific hemoglobin variants at www.ngsp.org.
More information about problems with the A1C test and different forms of sickle cell anemia is provided in the NIDDK health topics:
False A1C results may also occur in people with other problems that affect their blood or hemoglobin. For example, a falsely low A1C result can occur in people with
anemia
heavy bleeding
A falsely elevated A1C result can occur in people who
are very low in iron, for example, those with iron deficiency anemia
Other causes of false A1C results include
kidney failure
liver disease
How is the A1C test used after diagnosis of diabetes?
Health care providers can use the A1C test to monitor blood glucose levels in people with type 1 or type 2 diabetes. The A1C test is not used to monitor gestational diabetes.
The American Diabetes Association recommends that people with diabetes who are meeting treatment goals and have stable blood glucose levels have the A1C test twice a year. Health care providers may repeat the A1C test as often as four times a year until blood glucose levels reach recommended levels.
The A1C test helps health care providers adjust medication to reduce the risk of long-term diabetes complications. Studies have demonstrated substantial reductions in long-term complications with the lowering of A1C levels.
When the A1C test is used for monitoring blood glucose levels in a person with diabetes, the blood sample can be analyzed in a health care provider’s office using a POC test to give immediate results. However, POC tests are less reliable and not as accurate as most laboratory tests.
How does the A1C relate to estimated average glucose?
Estimated average glucose (eAG) is calculated from the A1C. Some laboratories report eAG with the A1C test results. The eAG number helps people with diabetes relate their A1C to daily glucose monitoring levels. The eAG calculation converts the A1C percentage to the same units used by home glucose meters—milligrams per deciliter (mg/dL).
The eAG number will not match daily glucose readings because it is a long-term average rather than the blood glucose level at a single time, as measured with the home glucose meter. The following table shows the relationship between the A1C and the eAG.
Relationship between A1C and eAG
Source: Adapted from American Diabetes Association. Standards of medical care in diabetes—2014.
Diabetes Care. 2014;37(Supp 1):S14–S80, table 8.
A1C
eAG
Percent
mg/dL
6
126
7
154
8
183
9
212
10
240
11
269
12
298
What A1C target should people have?
People will have different A1C targets depending on their diabetes history and their general health. People should discuss their A1C target with their health care provider. Studies have shown that people with diabetes can reduce the risk of diabetes complications by keeping A1C levels below 7 percent.
Maintaining good blood glucose control will benefit those with new-onset diabetes for many years to come. However, an A1C level that is safe for one person may not be safe for another. For example, keeping an A1C level below 7 percent may not be safe if it leads to problems with hypoglycemia, also called low blood glucose.
Less strict blood glucose control, or an A1C between 7 and 8 percent—or even higher in some circumstances—may be appropriate in people who have
limited life-expectancy
long-standing diabetes and difficulty attaining a lower goal
severe hypoglycemia
advanced diabetes complications such as chronic kidney disease, nerve problems, or cardiovascular disease
Will the A1C test show changes in blood glucose levels?
Large changes in a person’s blood glucose levels over the past month will show up in their A1C test result, but the A1C does not show sudden, temporary increases or decreases in blood glucose levels. Even though the A1C represents a long-term average, blood glucose levels within the past 30 days have a greater effect on the A1C reading than those in previous months.
Points to Remember
The A1C test is a blood test that provides information about a person’s average levels of blood glucose, also called blood sugar, over the past 3 months.
The A1C test is based on the attachment of glucose to hemoglobin, the protein in red blood cells that carries oxygen. Thus, the A1C test reflects the average of a person’s blood glucose levels over the past 3 months.
In 2009, an international expert committee recommended the A1C test be used as one of the tests available to help diagnose type 2 diabetes and prediabetes.
Because the A1C test does not require fasting and blood can be drawn for the test at any time of day, experts are hoping its convenience will allow more people to get tested—thus, decreasing the number of people with undiagnosed diabetes.
In the past, the A1C test was not recommended for diagnosis of type 2 diabetes and prediabetes because the many different types of A1C tests could give varied results. The accuracy has been improved by the National Glycohemoglobin Standardization Program (NGSP), which developed standards for the A1C tests. Blood samples analyzed in a health care provider’s office, known as point-of-care (POC) tests, are not standardized for use in diagnosing diabetes.
The A1C test may be used at the first visit to the health care provider during pregnancy to see if women with risk factors had undiagnosed diabetes before becoming pregnant. After that, the oral glucose tolerance test (OGTT) is used to test for diabetes that develops during pregnancy—known as gestational diabetes.
The standard blood glucose tests used for diagnosing type 2 diabetes and prediabetes—the fasting plasma glucose (FPG) test and the OGTT—are still recommended. The random plasma glucose test may be used for diagnosing diabetes when symptoms of diabetes are present.
The A1C test can be unreliable for diagnosing or monitoring diabetes in people with certain conditions that are known to interfere with the results.
The American Diabetes Association recommends that people with diabetes who are meeting treatment goals and have stable blood glucose levels have the A1C test twice a year.
Estimated average glucose (eAG) is calculated from the A1C to help people with diabetes relate their A1C to daily glucose monitoring levels.
People will have different A1C targets depending on their diabetes history and their general health. People should discuss their A1C target with their health care provider.
References
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Two Reasons I Find Time to Prevent Diabetes: My Future & Theirs (Tips for Asian Americans & Pacific Islanders)
This tip sheet can help Asian Americans and Pacific Islanders at risk for type 2 diabetes move more and eat less to lower their risk for diabetes.
Take these small steps now to prevent diabetes.
Find out if you are at risk.
Asian Americans and Pacific Islanders who are overweight are at high risk for type 2 diabetes or prediabetes - that means a person’s blood glucose levels are higher than normal, but not yet high enough to be called diabetes. Talk with your doctor about YOUR risk. To learn more, take the risk test on the other side of this tip sheet.
Lose a small amount of weight.
The weight you think is normal for you may not be a healthy weight. Check the chart on the other side to see if your weight puts you at risk for diabetes. You can prevent or delay type 2 diabetes by losing as little as 10 pounds.
Be more physically active.
Choose an activity you enjoy. Ask family members or friends to be active with you. Take a walk, swim, bike ride, dance, or play ball — together. Be active at least 30 minutes a day, 5 days a week to help you lose weight and stay healthy.
Make healthy food choices.
Choose more fruits and vegetables, fish, lean meats, whole grain rice, and low-fat or skim milk and cheese. Make healthy food choices as a family. Keep healthy snacks such as fruit in the house. Eat fewer fatty and fried foods. Serve smaller portions. Choose water to drink.
Record your progress.
Every day write down all the foods you eat and drink and the number of minutes you are active. Review it every day. Keeping a diary is one of the best ways to stay focused and reach your goals. NDEP’s GAME PLAN Food and Activity Tracker(PDF, 349 KB) can help.
Keep at it.
Add one new change each week. If you or your family members get off track, start again and keep going.
My blood pressure is 140/90 or higher, or I have been told that I have high blood pressure.
My cholesterol (lipid) levels are not normal. My HDL cholesterol (“good” cholesterol) is less than 35 or my triglyceride level is higher than 250.
Patches of skin around my neck and armpits appear dark, thick, and velvety. This is called acanthosis nigricans.
I have been told I have blood vessel problems affecting my heart, brain, or legs.
Keep in mind: As people get older, their risk for type 2 diabetes increases.
At-Risk Weight Charts
Find your height in the correct chart. If your weight is equal to or greater than the weight listed, you are at increased risk for type 2 diabetes.
If You Are Asian American At Risk BMI = 23
Height
Weight
4'10"
110
4'11"
114
5'0"
118
5'1"
122
5'2"
126
5'3"
130
5'4"
134
5'5"
138
5'6"
142
5'7"
146
5'8"
151
5'9"
155
5'10"
160
5'11"
165
6'0"
169
6'1"
174
6'2"
179
6'3"
184
6'4"
189
If You Are Pacific Islander At Risk BMI = 26
Height
Weight
4'10"
124
4'11"
128
5'0"
133
5'1"
137
5'2"
142
5'3"
146
5'4"
151
5'5"
156
5'6"
161
5'7"
166
5'8"
171
5'9"
176
5'10"
181
5'11"
186
6'0"
191
6'1"
197
6'2"
202
6'3"
208
6'4"
213
If You Are Not Asian American or Pacific Islander At Risk BMI = 25
Height
Weight
4'10"
119
4'11"
124
5'0"
128
5'1"
132
5'2"
136
5'3"
141
5'4"
145
5'5"
150
5'6"
155
5'7"
159
5'8"
164
5'9"
169
5'10"
174
5'11"
179
6'0"
184
6'1"
189
6'2"
194
6'3"
200
6'4"
205
Source: Adapted from Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report
The U.S. Department of Health and Human Services' National Diabetes Education Program (NDEP) is jointly sponsored by the National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC) with the support of more than 200 partner organizations.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
We Have the Power to Prevent Diabetes: Tips for American Indians & Alaska Natives
We are American Indians and Alaska Natives, and we have the power to prevent type 2 diabetes. Science has proven that we can prevent diabetes if we lose as little as 10 pounds by walking 30 minutes 5 days a week and making healthy food choices
"I know everyone can do it once they make up their mind. A lot of people out there know it runs in their family and they think ‘Okay, I’m going to get it.’ No, it is not so. You can prevent it. If I can do it, so can you."
Glenda Thomas Fifer Gila River Indian Community and Diabetes Prevention Program Participant
Here are 7 powerful steps you can take to get started today:
Move More. Get up, get out, and get moving. Walk, dance, bike ride, swim, or play ball with your friends or family. It doesn’t matter what you do as long as you enjoy it. Try different things to keep it fun.
"I found ways to work activity into my day. I walk for 10 minutes every morning. At night, my wife and I walk with our daughter." Tom John Seneca
Make Healthy Food Choices. Focus on eating less. Eat fiber-rich fruits and vegetables each day. Choose whole grain foods such as whole wheat bread and crackers, oatmeal, brown rice, and cereals. Cut down on fatty and fried foods. You still can have foods you enjoy, just eat smaller servings. Choose water to drink.
“I used to always go back for second helpings. Now, I leave the leftovers for another day. I think it’s working.” Josephine Malemute, RN Athabascan
Take Off Some Weight. Once you start eating less and moving more, you will lose weight. By losing just 10 pounds, you can cut your chances of getting diabetes.
“Since losing a few pounds, I feel better and have more energy to do the things I enjoy.” Loreli Decora Wimmebago Tribe of Nebraska
Set Goals You Can Meet. Start by making small changes. Try being active for 15 minutes a day this week. Then each week add 5 minutes until you build up to at least 30 minutes 5 days a week. Try to cut 150 calories out of your diet each day (that’s one can of soda!). Slowly reduce your calories over time. Talk to your health care team about your goals.
“When I first started walking, I could only go for about 10 minutes. Now I feel stronger and am able to walk 45 minutes every day” Jonathan Feather Eastern Band of Cherokee Indians
Record Your Progress. Write down all the things you eat and drink and the number of minutes you are active. Keeping a diary is one of the best ways to stay focused and reach your goals.
Keeping track of my activity allows me to see how I’m doing. By walking for 10 minutes at least 3 times a day, I’m able to get my 30 minutes in.” Lorraine Valdez, RN Isleta/Laguna Pueblos
Seek Help. You don’t have to prevent diabetes alone. Ask your family and friends to help you out. Involve them in your activities. You can help each other move more, eat less, and live a healthy life. Go for a walk together or play a pick-up game of basketball. Join a support group in your area to help you stay on track.
“After dinner I often take a walk with my family instead of watching TV.” Kelly Moore, MD Creek Nation of Oklahoma
Keep at It. Making even small changes is hard in the beginning. Try to add one new change a week. If you get off track, start again and keep at it.
“When I don’t think I have time to exercise, I just remember how important it is to be around for my family.” Ralph Forquera Juaneño Band of California Indians
We have the power to help our people and the generations to come. We have the Power to Prevent Diabetes." Yvette Roubideaux, MD Rosebud Sioux
Take your first step today. Talk to your healthcare team about your risk for type 2 diabetes and the small steps you can take to prevent it.
The U.S. Department of Health and Human Services’ National Diabetes Education Program (NDEP) is jointly sponsored by the National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC) with the support of more than 200 partner organizations.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Diabetes is a disease that occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes from the food you eat. Insulin, a hormone made by the pancreas, helps glucose from food get into your cells to be used for energy. Sometimes your body doesn’t make enough—or any—insulin or doesn’t use insulin well. Glucose then stays in your blood and doesn’t reach your cells.
Over time, having too much glucose in your blood can cause health problems. Although diabetes has no cure, you can take steps to manage your diabetes and stay healthy.
Sometimes people call diabetes “a touch of sugar” or “borderline diabetes.” These terms suggest that someone doesn’t really have diabetes or has a less serious case, but every case of diabetes is serious.
What are the different types of diabetes?
The most common types of diabetes are type 1, type 2, and gestational diabetes.
Type 1 diabetes
If you have type 1 diabetes, your body does not make insulin. Your immune system attacks and destroys the cells in your pancreas that make insulin. Type 1 diabetes is usually diagnosed in children and young adults, although it can appear at any age. People with type 1 diabetes need to take insulin every day to stay alive.
Type 2 diabetes
If you have type 2 diabetes, your body does not make or use insulin well. You can develop type 2 diabetes at any age, even during childhood. However, this type of diabetes occurs most often in middle-aged and older people. Type 2 is the most common type of diabetes.
Gestational diabetes
Gestational diabetes develops in some women when they are pregnant. Most of the time, this type of diabetes goes away after the baby is born. However, if you’ve had gestational diabetes, you have a greater chance of developing type 2 diabetes later in life. Sometimes diabetes diagnosed during pregnancy is actually type 2 diabetes.
As of 2015, 30.3 million people in the United States, or 9.4 percent of the population, had diabetes. More than 1 in 4 of them didn’t know they had the disease. Diabetes affects 1 in 4 people over the age of 65. About 90-95 percent of cases in adults are type 2 diabetes.1
Who is more likely to develop type 2 diabetes?
You are more likely to develop type 2 diabetes if you are age 45 or older, have a family history of diabetes, or are overweight. Physical inactivity, race, and certain health problems such as high blood pressure also affect your chance of developing type 2 diabetes. You are also more likely to develop type 2 diabetes if you have prediabetes or had gestational diabetes when you were pregnant. Learn more about risk factors for type 2 diabetes.
What health problems can people with diabetes develop?
Over time, high blood glucose leads to problems such as
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Type 2 diabetes prevention is proven, possible, and powerful. Taking small steps, such as eating less and moving more to lose weight, can help you prevent or delay type 2 diabetes and related health problems. The information below is based on the NIH-sponsored Diabetes Prevention Program (DPP) research study, which showed that people could prevent or delay type 2 diabetes even if they were at high risk for the disease.
Set a weight-loss goal
If you are overweight, the keys to preventing type 2 diabetes are to lose weight by choosing foods and drinks that are lower in calories, and to be more active. Set a weight-loss goal that you can reach. Try to lose at least 5 to 10 percent of your current weight within 6 months. For example, if you weigh 200 pounds, a 10 percent weight-loss goal means that you will try to lose 20 pounds. A good short-term goal is to lose 1 to 2 pounds per week.
Find your current weight in the first column to see how much weight you would need to lose for a 5-, 7-, or 10-percent weight loss. For example, if you weigh 200 pounds and want to lose 5 percent of your current weight, then you would need to lose 10 pounds.
Your current weight in pounds
Pounds to lose 5 percent of your weight
Pounds to lose 7 percent of your weight
Pounds to lose 10 percent of your weight
150
8
11
15
175
9
12
18
200
10
14
20
225
11
16
23
250
13
18
25
275
14
19
28
300
15
21
30
325
16
23
33
350
18
25
35
Calculate your weight-loss goal
Use the example below to learn how to calculate your exact weight-loss goal. In this example, the goal is for a 240-pound person to lose 5 percent of his or her weight.
As shown in the example above, a 240-pound person who wants to lose 5 percent of his or her weight would lose 12 pounds and weigh 228 pounds.
Step Number
Action
Result
Step 1
Weigh yourself to get your current weight.
"My weight is 240 pounds."
Step 2
Multiply your weight by the percent you want to lose.
"I want to lose 5 percent of my weight." 240 pounds (current weight) x .05 (5 percent weight loss) 12 pounds to lose
Step 3
Subtract the answer in Step 2 from your current weight.
Watch a video that explains how breaking down a goal into small steps can make achieving it easier.
Follow a healthy eating plan for weight loss
Research shows that you can prevent or delay type 2 diabetes by losing weight by following a low-fat, reduced-calorie eating plan and by being more active. Following an eating plan can help you reach your weight-loss goal. There are many ways to do this. Remember that the key to losing weight and preventing type 2 diabetes is to make lifelong changes that work for you. Many popular weight-loss plans promise “quick fixes” and haven’t been proven to work long-term or to prevent type 2 diabetes.
The four most important steps to eating healthy for weight loss are:
Eat smaller portions than you currently eat of foods that are high in calories, fat, and sugar.
Eat healthier foods in place of less-healthy choices.
Choose foods with less trans fat, saturated fat, and added sugars.
Drink water instead of drinks with sugar such as soda, sports drinks, and fruit juice.
Pay attention to portion sizes
Using the plate method can help you manage your portion sizes. Fill half of your plate with fruits and vegetables. Fill one quarter with a lean protein, such as chicken or turkey without the skin, or beans. Fill one quarter with a whole grain, such as brown rice or whole-wheat pasta.
Source: U.S. Department of Agriculture
You can use everyday objects or your hand to judge the size of a portion. For example:
1 serving of meat or poultry is about the size of the palm of your hand or a deck of cards
1 3-ounce serving of fish is the size of a checkbook
1 serving of cheese is like six dice
1/2 cup of cooked rice or pasta is like a rounded handful or a tennis ball
2 tablespoons of peanut butter is like a ping-pong ball
The table below shows how many calories and fat grams to eat each day to lose weight. Your needs may be different, but these are good starting points. The amounts are based on the eating patterns used in the Diabetes Prevention Program research study.
Your eating plan should include a variety of foods from each food group. Use this chart from the U.S. Department of Agriculture to learn more about which foods to eat.
Source: U.S. Department of Agriculture
Eating tips for weight loss
Try to get as close as possible to your daily calorie and fat gram goals.
Eat meals and snacks at about the same time each day to keep from getting too hungry.
Eat your meals on smaller plates and put your drinks in smaller glasses to make portions look bigger. Don’t worry about cleaning your plate.
Eat slowly. It takes 20 minutes for your stomach to send a signal to your brain that you are full.
Limit alcoholic beverages. If you drink alcohol, choose light beer or wine instead of mixed drinks.
Here are more tips on healthy eating.
Tips for eating at home
Use low-fat, light, or fat-free sour cream, cream cheese, mayonnaise, cheese, and salad dressing.
Cook with a mix of spices instead of salt.
Refrigerate extra portions of food right after cooking so that you’re less tempted to go back for seconds.
Freeze extra portions of food to have meals ready on days when you’re too busy or too tired to cook.
Share a bowl of fruit with family and friends instead of cookies or chips.
Eat fat-free or low-fat frozen yogurt or sherbet instead of ice cream.
Tips for eating at work or on the run
Take your lunch to work or meetings to stay in charge of what you eat.
Pack your lunch the night before so it’s ready to go when you are.
Make a sandwich on whole-grain bread with turkey or lean beef.
Use mustard or hummus instead of mayonnaise as a sandwich spread.
Add carrots and celery sticks to your lunch instead of chips.
Drink water instead of juice or regular soda.
Pack a snack like an apple or fat-free yogurt to eat if you get hungry.
Tips for eating in-between meals
Eat fruits, vegetables, or a small handful of unsalted nuts instead of chips or candy.
To reduce calories, drink water instead of regular soda, sports drinks, or juice.
Chew sugar-free gum between meals to help reduce your urge to snack.
Tips for food shopping
Make a list of what you need before going to the store, and stick to your list.
Eat a healthy snack or meal before shopping for food. Don’t shop on an empty stomach.
Compare nutrition facts on food labels and choose foods that are lower in calories, saturated fat, trans fats, and sodium.
Buy a new fruit or vegetable to try each time you go to the store. Use it to add flavor and color to soups, stews, or salads.
Buy reduced-fat or light versions of mayonnaise, cheese, and salad dressing.
Buy fat-free, low-fat, or soy milk instead of whole milk.
Tips for eating when dining out
When possible, plan ahead by looking at the menu and nutrition information online.
Take time when reading the menu to choose healthier meal options.
Order from a menu instead of a buffet, where it is harder to control how much you eat.
Ask about the portion size, amount of fat, and number of calories in menu items when deciding what to order.
Ask to have your meal prepared with less fat, salt, or added sugars.
Choose foods that are baked, steamed, grilled, or broiled instead of fried.
Choose healthier foods at fast food restaurants. Eat grilled chicken (without the skin) instead of a cheeseburger.
Order a salad for starters, and share your main dish with a friend or have the other half wrapped to go.
Order sauces, salad dressing, or spreads on the side to reduce the amount used on your meal.
Ask to have the amount you don’t want to eat put in a take-home container.
It’s okay to have a small portion of high-calorie foods once in a while. Just keep your weight-loss goal in mind.
Watch a short video about Latecia, who after seeing her mom live with diabetes, knew she needed to make changes in her life to prevent the disease.
Resources to learn more about choosing an eating plan for weight loss
When you move more every day, you will burn more calories. This can help you reach your weight-loss goal and keep the weight off. Even if you don’t lose weight, being more active may help you prevent or delay type 2 diabetes.
Find ways to be active for at least 30 minutes, 5 days a week. Walking is recommended for most people. Check with your health care team about other exercise programs.
Use these tips to get started, and keep moving:
Dress to move. Wear walking shoes that fit your feet and provide comfort and support. Your clothes should allow you to move and should keep you dry and comfortable. Look for fabrics that take sweat away from your skin to keep you cool.
Start slowly. Start by taking a 5-10 minute walk (or doing another activity that you like) on most days of the week. Slowly, add more time until you reach at least 30 minutes of moderate-intensity activity 5 days a week. Moderate-intensity activity will increase your heart rate and breathing. To check your intensity, use the Talk Test: a person doing moderate-intensity activity is able to talk but not sing.
Add more movement to your day. There are many ways you can add more movement to your day. If you have a dog, take your dog for a brisk walk in the morning or evening. When going shopping, park further away from the store’s entrance to increase your walk time. If you ride the bus, get off one stop early and walk the rest of the way if it is safe.
Try to sit less in your day. Get up every hour and move. When you watch TV, walk or dance around the room, march in place, or stretch.
Move more at work. Take a “movement break” during the day. Go for a walk during lunchtime. Deliver a message in person to a coworker instead of sending an email. Walk around your workplace while talking on the telephone. Take the stairs instead of the elevator to your workplace. Use the alarm on your phone, watch, or other device to remind you to take “movement breaks.”
Count your steps. You may be surprised to learn how much walking you already do every day. Use a pedometer or other wearable device to keep track of your steps. A pedometer is a gadget that counts the number of steps you take. Work up to 7, 000-10,000 steps per day.
Keep your muscles strong. Do activities to strengthen your muscles, such as lifting weights or using resistance bands 2 or more days a week.
Stretch it out. If your body aches or is sore, you are less likely to move more. To reduce stiff or sore muscles or joints, consider stretching after being active. Don’t bounce when you stretch. Perform slow movements and stretch only as far as you feel comfortable.
Make it social. When you bring other people into your activities, you are more likely to stick to your plan. Make walking “dates” with friends or family members throughout the week. For family fun, play soccer, basketball, or tag with your children. Take a class at a local gym or recreation center to be active with other people. Start a walking group with your neighbors, at work, or where you worship.
Have fun. Being active doesn’t have to be boring or painful. Turn up the music and dance while cleaning the house. Go dancing with friends and family members. Play sports with your kids or grandkids. Try swimming, biking, walking, jogging, or any activity that you enjoy that gets you moving. Find different ways to be active so you won’t get bored.
Keep at it. Reward yourself with nonfood treats, such as watching a movie, to celebrate your small successes. The longer you keep at it, the better you’ll feel. Making changes is never easy, but being more active is one small step toward a big reward: a healthier life.
Watch a video with physical activity tips and tips on taking small steps to become and stay more active.
Resources to learn how to get started with becoming more active
Go4Life—A campaign designed to help older adults fit activity into daily life.
Track your progress
Research shows that people who keep track of their weight and activity reach their goals more often than those who don’t. Weigh yourself at least once a week. Keep track of what you eat and drink, how many minutes of activity you get each day, and your weight.
The examples below show how to record your daily activity and food intake.
Daily Activity
Type of Activity
Minutes
Walking
10
Stationary bike
20
Daily Total
30
Daily Steps
Number of Steps Taken
7,450
Daily Food and Drink Intake
Time
Amount
Food Item
Calories
Fat Grams
8:00 a.m.
1 cup
Oatmeal
160
3.5
½ cup
Strawberries
25
0
6 oz.
Light yogurt
90
0
1 cup
Tea with sugar-free sweetener
0
0
11:00 a.m.
10
Almonds
70
6.0
12:30 p.m.
2 slices
Wheat bread
160
2.0
4 oz.
Ham
125
3.0
2 tsp.
Mustard
5
0
1 oz. slice
Cheese
110
9.0
1 oz.
Potato chips
160
10.0
10
Cherry tomatoes
30
0
4:00 p.m.
4 squares
Graham crackers
120
3.0
1 tbsp.
Peanut butter
95
8.0
6:30 p.m.
3 oz. skinless
Chicken breast
140
3.0
1 cup
Cooked broccoli
55
0
½ cup
Brown rice
110
1.0
1 cup
Pineapple chunks
80
0
1 cup
Nonfat milk
90
.5
Daily Total
1,625 calories
49.0 grams
Resources to record your meals and how much you move each day
You can also download an app to your smartphone or tablet that helps you track what you eat, your activity, and your weight.
Talk with your health care team
People are usually more successful at weight loss and being more active if they have regular contact and support from health professionals. Talk with your health care team about the changes you want to make to prevent type 2 diabetes.
Tell your health care team about your progress with weight loss and activity, and if you are having trouble sticking with your plan.
Ask your health care team if you should take a medicine called metformin. Research shows that taking metformin can help prevent or delay type 2 diabetes. It is most helpful in younger people who are overweight and have prediabetes, and for women who have had gestational diabetes, a type of diabetes that develops during pregnancy.
Contact your health insurance provider to learn what benefits are offered for weight-loss programs, diabetes-prevention programs, nutrition counseling, or fitness programs.
Some people with Medicare may be eligible for Intensive Behavioral Therapy for Obesity. This service includes up to 1 year of in-person weight-loss counseling visits with a health care professional.
If you smoke or use other tobacco products, you should stop. Even though quitting smoking can make it hard to manage your weight, it is a very important step to improve your health. Ask your health care team to help you create a plan for quitting. You can start by calling the national quitline at 1-800-QUITNOW (1-800-784-8669). For tips on quitting, go to SmokeFree.gov.
Get support for changing your lifestyle
Making big changes in your life is hard. You don’t have to change everything at once. You can make it easier by taking these steps:
Think about what is important to your health. What are you willing and able to do? Example: I know that being more active can help me lose some weight.
Decide what your goals are. Choose one goal to work on first. Example: I want to see if I can work up to getting 30 minutes of walking in a day on at least 5 days of the week.
Decide what steps will help you reach your goal.
Steps to reach your goal
Example
Set a time frame and deadline for making lifestyle changes.
I’ll start this week by walking for 10 minutes at lunch time.
Plan what you need to get ready.
I need to take walking shoes to work.
Think about what might prevent you from reaching your goals.
In bad weather, I won’t want to walk outside. I can walk inside instead.
Decide how you will reward yourself when you do what you have planned.
If I stick with my plans this week, I’ll watch a movie.
Pick one step to try this week.
Add one or two healthy changes every week. Don’t get upset with yourself if you have a setback or lose control of your plan. Everyone has slips. Injury, illness, or being too busy can make it hard to stick to your plan. It’s not easy to make lifelong changes in what you eat and drink and in how often you are active. The important thing is to review your Game Plan and get back on track as soon as possible.
Resources to plan your lifestyle changes
Diabetes HealthSense: Make a Plan—online or printable tool asks questions to help you consider what is important to you about your health
Find family and friends who will support and encourage you in preventing type 2 diabetes. Join with a neighbor or coworker in changing your lifestyle. Talk with your health care team to learn about programs that may help, such as the National Diabetes Prevention Program.
National Diabetes Prevention Program—Led by the Centers for Disease Control and Prevention (CDC), the National Diabetes Prevention Program offers lifestyle change programs based on the Diabetes Prevention Program research study. Participants work with a lifestyle coach in a live group or online setting to receive a 1-year lifestyle change program that includes 16 core sessions (usually 1 per week) and 6 post-core sessions (1 per month). Find a program near you.
Local hospitals, health departments, libraries, senior centers, or faith-based organizations may offer additional programs or seminars about type 2 diabetes prevention.
The U.S. Department of Health and Human Services’ National Diabetes Education Program (NDEP) is jointly sponsored by the National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC) with the support of more than 200 partner organizations.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.



 marks in this booklet show actions you can take to manage your diabetes.
marks in this booklet show actions you can take to manage your diabetes. Actions you can take
Actions you can take