Cystoscopy & UreteroscopyWhat are cystoscopy and ureteroscopy?Cystoscopy and ureteroscopy are common procedures performed by a urologist to look inside the urinary tract. A urologist is a doctor who specializes in urinary tract problems. Cystoscopy. Cystoscopy uses a cystoscope to look inside the urethra and bladder. A cystoscope is a long, thin optical instrument with an eyepiece at one end, a rigid or flexible tube in the middle, and a tiny lens and light at the other end of the tube. By looking through the cystoscope, the urologist can see detailed images of the lining of the urethra and bladder. The urethra and bladder are part of the urinary tract. Ureteroscopy. Ureteroscopy uses a ureteroscope to look inside the ureters and kidneys. Like a cystoscope, a ureteroscope has an eyepiece at one end, a rigid or flexible tube in the middle, and a tiny lens and light at the other end of the tube. However, a ureteroscope is longer and thinner than a cystoscope so the urologist can see detailed images of the lining of the ureters and kidneys. The ureters and kidneys are also part of the urinary tract. 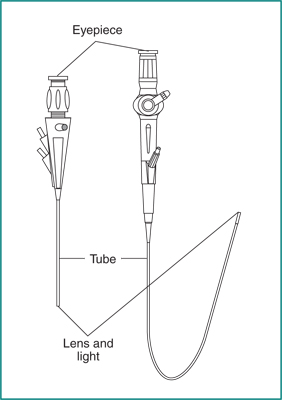
What is the urinary tract and how does it work?The urinary tract is the body’s drainage system for removing urine, which is composed of wastes and extra fluid. In order for normal urination to occur, all body parts in the urinary tract need to work together in the correct order. Kidneys. The kidneys are two bean-shaped organs, each about the size of a fist. They are located just below the rib cage, one on each side of the spine. Every day, the kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine. The kidneys work around the clock; a person does not control what they do. Ureters. Ureters are the thin tubes of muscle—one on each side of the bladder—that carry urine from each of the kidneys to the bladder. Bladder. The bladder, located in the pelvis between the pelvic bones, is a hollow, muscular, balloon-shaped organ that expands as it fills with urine. Although a person does not control kidney function, a person does control when the bladder empties. Bladder emptying is known as urination. The bladder stores urine until the person finds an appropriate time and place to urinate. A normal bladder acts like a reservoir and can hold 1.5 to 2 cups of urine. How often a person needs to urinate depends on how quickly the kidneys produce the urine that fills the bladder. The muscles of the bladder wall remain relaxed while the bladder fills with urine. As the bladder fills to capacity, signals sent to the brain tell a person to find a toilet soon. During urination, the bladder empties through the urethra, located at the bottom of the bladder. Three sets of muscles work together like a dam, keeping urine in the bladder. The first set is the muscles of the urethra itself. The area where the urethra joins the bladder is the bladder neck. The bladder neck, composed of the second set of muscles known as the internal sphincter, helps urine stay in the bladder. The third set of muscles is the pelvic floor muscles, also referred to as the external sphincter, which surround and support the urethra. To urinate, the brain signals the muscular bladder wall to tighten, squeezing urine out of the bladder. At the same time, the brain signals the sphincters to relax. As the sphincters relax, urine exits the bladder through the urethra. 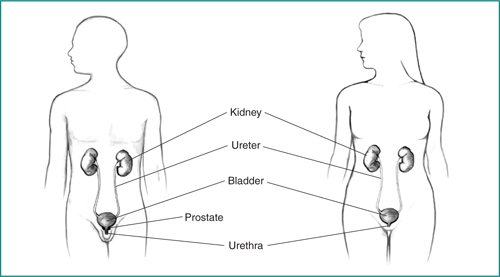
Why is a cystoscopy or ureteroscopy performed?A urologist performs a cystoscopy or ureteroscopy to find the cause of, and sometimes treat, urinary tract problems. Cystoscopy. A urologist performs a cystoscopy to find the cause of urinary tract problems such as
During a cystoscopy, a urologist can see
During a cystoscopy, a urologist can treat problems such as bleeding in the bladder and blockage in the urethra. A urologist may also use a cystoscopy to
Ureteroscopy. In addition to the causes of urinary tract problems he or she can find with a cystoscope, a urologist performs a ureteroscopy to find the cause of urine blockage in a ureter or to evaluate other abnormalities inside the ureters or kidneys. During a ureteroscopy, a urologist can see
During a ureteroscopy, a urologist can treat problems such as urine blockage in a ureter. The urologist can also
After a ureteroscopy, the urologist may need to place a stent in a ureter to drain urine from the kidney to the bladder while swelling in the ureter goes away. The stent, which is completely inside the body, may cause some discomfort in the kidney or bladder area. The discomfort is generally mild. The stent may be left in the ureter for a few days to a week or more. The urologist may need to perform a cystoscopy to remove the stent in the ureter. How does a patient prepare for a cystoscopy or ureteroscopy?In many cases, a patient does not need special preparations for a cystoscopy. A health care provider may ask the patient to drink plenty of liquids before the procedure, as well as urinate immediately before the procedure. The patient may need to give a urine sample to test for a UTI. If the patient has a UTI, the urologist may treat the infection with antibiotics before performing a cystoscopy or ureteroscopy. A health care provider will provide instructions before the cystoscopy or ureteroscopy. These instructions may include
The urologist will ask about the patient’s medical history, current prescription and over-the-counter medications, and allergies to medications, including anesthetics. The urologist will talk about which anesthetic is best for the procedure and explain what the patient can expect after the procedure. How is a cystoscopy or ureteroscopy performed?A urologist performs a cystoscopy or ureteroscopy during an office visit or in an outpatient center or a hospital. For some patients, the urologist will apply an anesthetic gel around the urethral opening or inject a local anesthetic into the urethra. Some patients may require sedation or general anesthesia. The urologist often gives patients sedatives and general anesthesia for a
For sedation and general anesthesia, a nurse or technician places an intravenous (IV) needle in a vein in the arm or hand to give the medication. Sedation helps the patient relax and be comfortable. General anesthesia puts the patient into a deep sleep during the procedure. The medical staff will monitor the patient’s vital signs and try to make him or her as comfortable as possible. During both procedures, a woman will lie on her back with the knees up and spread apart. During a cystoscopy, a man can lie on his back or be in a sitting position. After the anesthetic has taken effect, the urologist gently inserts the tip of the cystoscope or ureteroscope into the urethra and slowly glides it through the urethra and into the bladder. A sterile liquid—water or salt water, called saline—flows through the cystoscope or ureteroscope to slowly fill the bladder and stretch it so the urologist has a better view of the bladder wall. As the bladder fills with liquid, the patient may feel some discomfort and the urge to urinate. The urologist may remove some of the liquid from the bladder during the procedure. As soon as the procedure is over, the urologist may remove the liquid from the bladder or the patient may empty the bladder. For a cystoscopy, the urologist examines the lining of the urethra as he or she passes the cystoscope into the bladder. The urologist then examines the lining of the bladder. The urologist can insert small instruments through the cystoscope to treat problems in the urethra and bladder or perform a biopsy. For a ureteroscopy, the urologist passes the ureteroscope through the bladder and into a ureter. The urologist then examines the lining of the ureter. He or she may pass the ureteroscope all the way up into the kidney. The urologist can insert small instruments through the ureteroscope to treat problems in the ureter or kidney or perform a biopsy. When a urologist performs a cystoscopy or a ureteroscopy to make a diagnosis, both procedures—including preparation—take 15 to 30 minutes. The time may be longer if the urologist removes a stone in the bladder or a ureter or if he or she performs a biopsy. What can a patient expect after a cystoscopy or ureteroscopy?After a cystoscopy or ureteroscopy, a patient may
These problems should not last more than 24 hours. The patient should tell a health care provider right away if bleeding or pain is severe or if problems last more than a day. The health care provider may recommend that the patient
The health care provider may prescribe an antibiotic to take for 1 or 2 days to prevent an infection. A patient should report any signs of infection—including severe pain, chills, or fever—right away to the health care provider. Most patients go home the same day as the procedure. Recovery depends on the type of anesthesia. A patient who receives only a local anesthetic can go home immediately. A patient who receives general anesthesia may have to wait 1 to 4 hours before going home. A health care provider usually asks the patient to urinate before leaving. In some cases, the patient may need to stay overnight in the hospital. A health care provider will provide discharge instructions for rest, driving, and physical activities after the procedure. What are the risks of cystoscopy and ureteroscopy?The risks of cystoscopy and ureteroscopy include
Points to Remember
Clinical TrialsThe National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions. What are clinical trials, and are they right for you?Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you. What clinical trials are open?Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov. This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts. The NIDDK would like to thank: Syndicated Content Details: Source URL: https://www.niddk.nih.gov/Syndication/cystoscopy-ureteroscopy Source Agency: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Captured Date: 2016-04-25 21:25:00.0 Urinary Tract ImagingWhat is the urinary tract?The urinary tract is the body’s drainage system for removing wastes and extra water. The urinary tract includes two kidneys, two ureters, a bladder, and a urethra. The kidneys are a pair of bean-shaped organs, each about the size of a fist and located below the ribs, one on each side of the spine, toward the middle of the back. Every minute, a person’s kidneys filter about 3 ounces of blood, removing wastes and extra water. The wastes and extra water make up the 1 to 2 quarts of urine an adult produces each day. Children produce less urine each day; the amount produced depends on their age. The urine travels from the kidneys down two narrow tubes called the ureters. The urine is then stored in a balloonlike organ called the bladder. When the bladder empties, urine flows out of the body through a tube called the urethra at the bottom of the bladder. 
What does “imaging” mean?In medicine, “imaging” is the general term for any technique used to provide pictures of bones and organs inside the body. Imaging techniques include conventional radiology, or x-rays; ultrasound; magnetic resonance imaging (MRI); computerized tomography (CT) scans; and radionuclide scans. Imaging helps the health care provider see the causes of medical problems. What problems could require imaging of the urinary tract?Imaging can help the health care provider find the cause of
One symptom can have several possible causes. The health care provider can use imaging techniques to determine, for example, whether a urinary tract stone or an enlarged prostate is blocking urine flow. Imaging can help clarify kidney diseases, tumors, urinary tract infections (UTIs), urinary retention, small bladder capacity, and urinary reflux—the backward flow of urine. What steps does the health care provider take before ordering imaging tests?Before ordering imaging tests, the health care provider
These steps help the health care provider determine the possible causes of the urinary tract problems and what to look for in an imaging test. What are the imaging techniques?The health care provider can use several different imaging techniques depending on factors such as the person’s general medical history and urinary tract symptoms. Conventional RadiologyX-ray machines have been used to diagnose diseases for about 100 years. X-rays of the urinary tract can help highlight a kidney stone or tumor that could be blocking the flow of urine and causing pain. For men, an x-ray also shows the size and shape of the prostate—a walnut-shaped gland that surrounds the urethra at the neck of the bladder and supplies fluid that goes into semen. Conventional x-rays do involve some exposure to ionizing radiation—radiation that is strong enough to damage some cells. Two common x-ray procedures include the injection of a special dye, called contrast medium, which shows the shape of the urinary tract. Intravenous pyelogram (IVP). An IVP is an x-ray of the urinary tract. Contrast medium is injected into a vein in the person’s arm, travels through the body to the kidneys, and makes urine visible on the x-ray. The contrast medium also shows any blockage in the urinary tract. The procedure is performed in a health care provider’s office, outpatient center, or hospital by an x-ray technician, and the images are interpreted by a radiologist—a doctor who specializes in medical imaging; anesthesia is not needed. An IVP can help locate problems in the kidneys, ureters, or bladder that may be caused by urinary retention or reflux. 
Voiding cystourethrogram (VCUG). A VCUG is an x-ray image of the bladder and urethra taken while the bladder is full and during urination, also called voiding. As the person lies on the x-ray table, a health care provider inserts the tip of a thin, flexible tube called a catheter through the urethra into the bladder. The bladder is filled with contrast medium to make it clearly visible on the x-ray images. The x-rays are taken from various angles while the bladder is full of contrast medium. The catheter is then removed and x-ray images are taken during urination. The procedure is performed in a health care provider’s office, outpatient center, or hospital by an x-ray technician. The technician is supervised by a radiologist while the images are taken. The radiologist then interprets the images. Anesthesia is not needed, but sedation may be used for some people. A VCUG can reveal abnormalities of the inside of the urethra and bladder and is usually used for children to detect vesicoureteral reflux—the abnormal flow of urine from the bladder back into the upper urinary tract. A VCUG can also show whether the flow of urine is normal when the bladder empties, blockages from an enlarged prostate in men, and an abnormal bladder position in women. UltrasoundUltrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. The transducer can be moved to different angles to make it possible to examine different organs. The procedure is performed in a health care provider’s office, outpatient center, or hospital by a specially trained technician, and the images are interpreted by a radiologist; anesthesia is not needed. The images can be used to provide information that is valuable in diagnosing and treating a variety of diseases and conditions. Abdominal ultrasound. In abdominal ultrasound, the health care provider applies a gel to the person’s abdomen and moves a hand-held transducer over the skin. The gel allows the transducer to glide easily, and it improves the transmission of the signals. The procedure is performed in a health care provider’s office, outpatient center, or hospital by a specially trained technician, and the images are interpreted by a radiologist; anesthesia is not needed. An abdominal ultrasound can create images of the entire urinary tract. The images can show damage or abnormalities in the urinary tract. Abdominal ultrasounds are also commonly used to take pictures of fetuses in the womb and of a woman’s ovaries and uterus. Transrectal ultrasound with prostate biopsy. Transrectal ultrasound is most often used to examine the prostate. In a transrectal ultrasound, the health care provider inserts a transducer slightly larger than a pen into the man’s rectum next to the prostate. The ultrasound image shows the size of the prostate and any abnormal-looking areas, such as tumors. Transrectal ultrasound cannot be used to definitively diagnose prostate cancer. To determine whether a tumor is cancerous, the health care provider performs a biopsy. For the biopsy, the health care provider uses the transducer and ultrasound images to guide a needle to the prostate. The needle is then used to remove a few pieces of prostate tissue for examination with a microscope. A transrectal ultrasound with prostate biopsy is usually performed in a health care provider’s office, outpatient facility, or hospital by a doctor; light sedation and local anesthesia are used. The biopsied prostate tissue is examined in a laboratory by a pathologist—a doctor who specializes in diagnosing diseases. The biopsy can reveal whether prostate cancer is present. 
MRIMagnetic resonance imaging is a test that takes pictures of the body’s internal organs and soft tissues without using x-rays. MRI machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues. An MRI may include the injection of contrast medium. With most MRI machines, the person lies on a table that slides into a tunnel-shaped device where the images are taken. The device may be open ended or closed at one end; some newer machines are designed to allow the person to lie in a more open space. During an MRI, the person is usually awake but must remain perfectly still while the images are being taken. A sequence of images taken from different angles may be needed to create a detailed picture of the urinary tract. During the sequencing, the person will hear loud, mechanical knocking and humming noises. The procedure is performed in an outpatient center or hospital by a specially trained technician, and the images are interpreted by a radiologist; anesthesia is not needed, though light sedation may be used for people with a fear of confined spaces. 
Magnetic resonance angiogram (MRA). An MRA is a type of MRI that provides the most detailed view of kidney arteries—the blood vessels that supply blood to the kidneys. An MRA can show kidney artery stenosis, which is the narrowing of a kidney artery that restricts blood flow to the kidney. Kidney artery stenosis can cause high blood pressure and lead to reduced kidney function and eventually kidney failure. CT ScansComputerized tomography scans use a combination of x-rays and computer technology to create three-dimensional (3-D) images. A CT scan may include the injection of contrast medium. CT scans require the person to lie on a table that slides into a tunnel-shaped device where the x-rays are taken. The procedure is performed in an outpatient center or hospital by a specially trained technician, and the images are interpreted by a radiologist; anesthesia is not needed. CT scans can show stones in the urinary tract, obstructions, infections, cysts, tumors, and traumatic injuries. 
Radionuclide ScansA radionuclide scan is an imaging technique that relies on the detection of small amounts of radiation after injection of radioactive chemicals. Because the dose of the radioactive chemicals is small, the risk of causing damage to cells is low. Special cameras and computers are used to create images of the radioactive chemicals as they pass through the urinary tract. Radionuclide scans are performed at a health care provider’s office, outpatient center, or hospital by a specially trained technician, and the images are interpreted by a radiologist; anesthesia is not needed. Radioactive chemicals injected into the blood can provide information about kidney function. Radioactive chemicals can also be put into the fluids used to fill the bladder and urethra for x-ray, MRI, and CT imaging. What preparations are needed for an imaging test?Preparations for an imaging test mostly depend on the purpose and type of test. In general, the health care provider will want to know whether the person is allergic to any foods or medications, is pregnant, or has had any recent illnesses or medical conditions. Specific preparations could include any of the following:
People undergoing an imaging test should listen to the health care provider’s instructions carefully and ask questions if something is not understood. What happens after imaging tests?After most imaging tests, the person can immediately resume normal activity. Tests that involved placing a catheter in the urethra may produce some mild discomfort for a few hours after the procedure. Drinking an 8-ounce glass of water every half-hour for 2 hours may help reduce the discomfort. The health care provider may recommend taking a warm bath or holding a warm, damp washcloth over the urethral opening to relieve the discomfort. A transrectal ultrasound may produce some discomfort. A prostate biopsy may produce pain in the area of the rectum and the perineum, which is between the rectum and the scrotum. A prostate biopsy may also produce blood in the urine and semen. For catheterization or biopsy, the health care provider may prescribe an antibiotic for 1 or 2 days to prevent an infection. People with signs of infection—including pain, chills, or fever—should call a health care provider immediately. Some people have reactions to the contrast medium or the sedatives, though the risks are generally low. Signs of contrast medium reactions include hives, itching, nausea, vomiting, headache, and dizziness. Contrast medium can cause kidney damage in people with certain conditions, such as impaired kidney function and diabetes. In most people, the kidney damage has no symptoms and goes away within a week or so. In rare cases, contrast medium causes lasting kidney damage. Signs of kidney damage include
Reactions to sedatives are rare but possible. Signs of sedative reactions include changes in breathing and heart rate. People with signs of reactions to the contrast medium or the sedatives should call a health care provider immediately. How soon will test results be available?The results of simple tests such as x-rays and abdominal ultrasound can be discussed with the health care provider soon after the test. Results of other tests such as a prostate tissue biopsy, MRI, and CT scans may take several days to come back. The health care provider will talk with the patient about these results. Points to Remember
Clinical TrialsThe National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions. What are clinical trials, and are they right for you?Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you. What clinical trials are open?Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov. This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts. The NIDDK would like to thank: Syndicated Content Details: Source URL: https://www.niddk.nih.gov/Syndication/urinary-tract-imaging Source Agency: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Captured Date: 2016-04-26 12:58:00.0 Prostate TestsWhat is the prostate?The prostate is a walnut-shaped gland that is part of the male reproductive system. It has two or more lobes, or sections, enclosed by an outer layer of tissue. The prostate is located in front of the rectum and just below the bladder, where urine is stored. It surrounds the urethra at the neck of the bladder and supplies fluid that goes into semen. 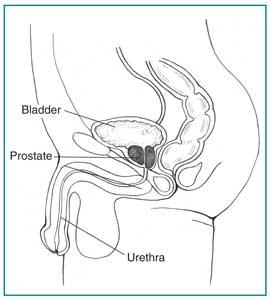
What are some common prostate problems?The most common prostate problem in men younger than age 50 is inflammation, called prostatitis. Prostate enlargement, or benign prostatic hyperplasia (BPH), is another common problem. Because the prostate continues to grow as a man ages, BPH is the most common prostate problem for men older than age 50. Older men are at risk for prostate cancer as well, but it is much less common than BPH. What are the symptoms of prostate problems?The symptoms of prostate problems may include
Different prostate problems may have similar symptoms. For example, one man with prostatitis and another with BPH may both experience urinary urgency. Sometimes symptoms for the same prostate problem differ among individuals. For example, one man with BPH may have trouble beginning a urine stream, while another may experience nocturia. A man in the early stages of prostate cancer may have no symptoms at all. Because of this confusing array of symptoms, a thorough medical exam and testing are vital. How are prostate problems diagnosed?To diagnose prostate problems, the health care provider will perform a digital rectal exam (DRE). The health care provider will also ask the patient
Answers to these questions will help the health care provider identify the problem or determine what medical tests are needed. Diagnosing BPH may require a series of medical exams and tests. How is a digital rectal exam (DRE) performed?A DRE is a physical exam of the prostate. The health care provider will ask the patient to bend over a table or lie on his side while holding his knees close to his chest. The health care provider slides a gloved, lubricated finger into the rectum and feels the part of the prostate that lies next to it. The DRE may be slightly uncomfortable, but it is brief. This exam reveals whether the prostate has any abnormalities that require more testing. If an infection is suspected, the health care provider might massage the prostate during the DRE to obtain fluid to examine with a microscope. This exam is usually done first. Many health care providers perform a DRE as part of a routine physical exam for men age 50 or older, some even at age 40, whether or not the man has urinary problems. 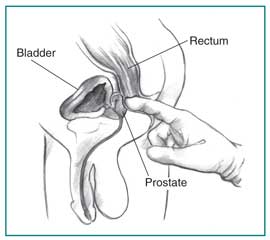
What is the first test for detecting prostate problems?The first test for detecting prostate problems is a blood test to measure prostate-specific antigen (PSA), a protein made only by the prostate gland. This test is often included in routine physical exams for men older than age 50. Because African American men have higher rates of getting, and dying from, prostate cancer than men of other racial or ethnic groups in the United States, medical organizations recommend a PSA blood test be given starting at age 40 for African American men. Medical organizations also recommend a PSA blood test be given starting at age 40 for men with a family history of prostate cancer. Some medical organizations even recommend a PSA blood test be given to all men starting at age 40. If urination problems are present or if a PSA blood test indicates a problem, additional tests may be ordered. These tests may require a patient to change his diet or fluid intake or to stop taking medications. If the tests involve inserting instruments into the urethra or rectum, antibiotics may be given before and after the test to prevent infection. Why is a prostate-specific antigen (PSA) blood test performed?A PSA blood test is performed to detect or rule out prostate cancer. The amount of PSA in the blood is often higher in men who have prostate cancer. However, an elevated PSA level does not necessarily indicate prostate cancer. The U.S. Food and Drug Administration has approved the PSA blood test for use in conjunction with a DRE to help detect prostate cancer in men age 50 or older and for monitoring men with prostate cancer after treatment. However, much remains unknown about how to interpret a PSA blood test, its ability to discriminate between cancer and problems such as BPH and prostatitis, and the best course of action if the PSA level is high. When done in addition to a DRE, a PSA blood test enhances detection of prostate cancer. However, the test is known to have relatively high false-positive rates. A PSA blood test also may identify a greater number of medically insignificant lumps or growths, called tumors, in the prostate. Health care providers and patients should weigh the benefits of PSA blood testing against the risks of follow-up diagnostic tests. The procedures used to diagnose prostate cancer may cause significant side effects, including bleeding and infection. What are additional tests for detecting prostate problems?If the DRE or the PSA blood test indicates a problem may exist, the health care provider may order additional tests, including urinalysis, urodynamic tests, cystoscopy, abdominal ultrasound, transrectal ultrasound with prostate biopsy, and imaging studies such as magnetic resonance imaging (MRI) or computerized tomography (CT) scan. UrinalysisUrinalysis is the testing of a urine sample for abnormal substances or signs of infection. The urine sample is collected in a special container in a health care provider’s office or commercial facility and can be tested in the same location or sent to a lab for analysis. If an infection is suspected, the health care provider may ask that the urine sample be collected in two or three containers during a single urination to help locate the infection site. After the first collection, the health care provider will have the patient stop the urine stream for a prostate massage before collecting more urine. If signs of infection appear in the first container but not in the others, the infection is likely to be in the urethra. If the urine contains significantly more bacteria after the prostate massage or bacteria are in the prostate fluid itself, the infection is likely to be in the prostate. Urodynamic TestsUrodynamic testing is any procedure that looks at how well the bladder, sphincters, and urethra are storing and releasing urine. Most urodynamic tests focus on the bladder’s ability to hold urine and empty steadily and completely. If the prostate problem appears to be related to urine blockage, the health care provider may recommend tests that measure bladder pressure and urine flow rate. One test involves urinating into a special device that measures how quickly the urine is flowing and records how many seconds it takes for the peak flow rate to be reached. Another test measures postvoid residual, the amount of urine left in the bladder when urination stops. A weak urine stream and urinary retention may be signs of urine blockage caused by an enlarged prostate that is squeezing the urethra. Some urodynamic tests are performed in a health care provider’s office without anesthesia. Other urodynamic tests are performed in a health care provider’s office, outpatient center, or hospital with local anesthesia. CystoscopyCystoscopy is a procedure that allows the health care provider to look for blockage in the lower urinary tract. A cystoscope is a tubelike instrument used to look inside the urethra and bladder. After a solution numbs the inside of the penis, the health care provider inserts the cystoscope through the opening at the tip of the penis and into the lower urinary tract. By looking through the cystoscope, the health care provider can determine the location and degree of the urine blockage. A cystoscopy is performed in a health care provider’s office, outpatient center, or hospital with local anesthesia. The procedure is usually performed by a urologist, a doctor who specializes in treating problems of the urinary tract and the male reproductive system. Abdominal UltrasoundUltrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. The transducer can be moved to different angles to make it possible to examine different organs. In abdominal ultrasound, the health care provider applies a gel to the patient’s abdomen and moves a handheld transducer over the skin. The gel allows the transducer to glide easily, and it improves the transmission of the signals. The procedure is performed in a health care provider’s office, outpatient center, or hospital by a specially trained technician and interpreted by a doctor, usually a radiologist—a doctor who specializes in medical imaging. Anesthesia is not needed. An abdominal ultrasound can create images of the entire urinary tract. The images can show damage or abnormalities in the urinary tract resulting from urine blockage at the prostate. Transrectal Ultrasound with Prostate BiopsyTransrectal ultrasound is most often used to examine the prostate. In a transrectal ultrasound, the health care provider inserts a transducer slightly larger than a pen into the man’s rectum next to the prostate. The ultrasound image shows the size of the prostate and any abnormal-looking areas, such as tumors. Transrectal ultrasound cannot definitively identify prostate cancer. To determine whether a tumor is cancerous, the health care provider uses the transducer and ultrasound images to guide a needle to the tumor. The needle is then used to remove a few pieces of prostate tissue for examination with a microscope. This process, called biopsy, can reveal whether prostate cancer is present. A transrectal ultrasound with prostate biopsy is usually performed by a doctor in a health care provider’s office, outpatient center, or hospital with light sedation and local anesthesia. The biopsied prostate tissue is examined in a laboratory by a pathologist—a doctor who specializes in diagnosing diseases. 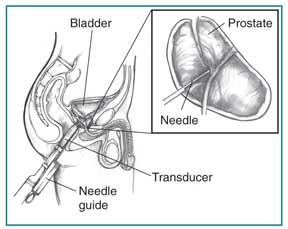
MRI and CT ScanAn MRI is a test that takes pictures of the body’s internal organs and soft tissues without using x-rays. The MRI machines use radio waves and magnets to produce detailed pictures. An MRI may also involve the injection of dye. A CT scan uses a combination of x-rays and computer technology to create three-dimensional (3-D) images. A CT scan may also involve the injection of a dye. MRI and CT scan images can help identify abnormal structures in the urinary tract, but they cannot distinguish between cancerous tumors and noncancerous prostate enlargement. Once a biopsy has confirmed cancer, these imaging techniques will show how far the cancer has spread. MRIs and CT scans are usually performed at an outpatient center or hospital by a specially trained technician and interpreted by a radiologist; anesthesia is not needed. For an MRI, light sedation may be used for people with a fear of confined spaces. What happens after the prostate tests?Urodynamic tests and cystoscopy may cause mild discomfort for a few hours after the procedures. Drinking an 8-ounce glass of water every half-hour for 2 hours may help reduce discomfort. The health care provider may recommend taking a warm bath or holding a warm, damp washcloth over the urethral opening to relieve discomfort. A prostate biopsy may produce pain in the area of the rectum and the perineum, which is between the rectum and the scrotum. A prostate biopsy may also produce blood in urine and semen. An antibiotic may be prescribed for 1 or 2 days to prevent infection. Patients with signs of infection—including pain, chills, or fever—should call their health care provider immediately. How soon will prostate test results be available?Results for simple medical tests such as some urodynamic tests, cystoscopy, and abdominal ultrasound are often available soon after the test. The results of other medical tests such as PSA blood test and prostate tissue biopsy may take several days to come back. A health care provider will talk with the patient about the results and possible treatments for the problem. Eating, Diet, and NutritionEating, diet, and nutrition have not been shown to play a role in causing or preventing prostate problems. Points to Remember
Clinical TrialsThe National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions. What are clinical trials, and are they right for you?Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you. What clinical trials are open?Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov. This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts. The NIDDK would like to thank: Syndicated Content Details: Source URL: https://www.niddk.nih.gov/Syndication/prostate Source Agency: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Captured Date: 2016-04-25 20:47:00.0 Urodynamic TestingWhat is the urinary tract?The urinary tract is the body’s drainage system for removing wastes and extra water. The urinary tract includes two kidneys, two ureters, a bladder, and a urethra. Blood flows through the kidneys, and the kidneys filter out wastes and extra water, making urine. The urine travels down two narrow tubes called the ureters. The urine is then stored in a muscular, balloonlike organ called the bladder. The bladder swells into a round shape when it is full and gets smaller as it empties. When the bladder empties, urine flows out of the body through the urethra. What is the lower urinary tract and how does it work?The lower urinary tract includes the bladder and urethra. The bladder sits in the pelvis and is attached to other organs, muscles, and the pelvic bones, which hold it in place. The urethra is a tube at the bottom of the bladder that carries urine from the bladder to the outside of the body. The lower urinary tract works by coordinating the muscles of the bladder wall with the sphincters, which are circular muscles that surround the area of the bladder that opens into the urethra. The muscles of the bladder wall relax as the bladder fills with urine. If the urinary tract is healthy, the bladder can hold up to 2 cups, or 16 ounces, of urine comfortably for 2 to 5 hours. The sphincters close tightly like rubber bands around the bladder to help keep urine from leaking. As the bladder fills, the need to urinate becomes stronger and stronger, until the bladder reaches its limit. Urination is the process of emptying the bladder. To urinate, the brain signals the bladder muscles to tighten, squeezing urine out of the bladder. At the same time, the brain signals the sphincters to relax. As the sphincters relax, urine exits the bladder through the urethra. When all the signals occur in the correct order, normal urination occurs. More information about the urinary tract and urinary tract problems is provided in the NIDDK health topic, The Urinary Tract and How It Works. 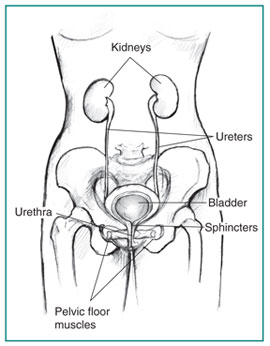
What is urodynamic testing?Urodynamic testing is any procedure that looks at how well the bladder, sphincters, and urethra are storing and releasing urine. Most urodynamic tests focus on the bladder’s ability to hold urine and empty steadily and completely. Urodynamic tests can also show whether the bladder is having involuntary contractions that cause urine leakage. A health care provider may recommend urodynamic tests if symptoms suggest problems with the lower urinary tract. Lower urinary tract symptoms (LUTS) include
Urodynamic tests range from simple observation to precise measurements using sophisticated instruments. For simple observation, a health care provider may record the length of time it takes a person to produce a urinary stream, note the volume of urine produced, and record the ability or inability to stop the urine flow in midstream. For precise measurements, imaging equipment takes pictures of the bladder filling and emptying, pressure monitors record the pressures inside the bladder, and sensors record muscle and nerve activity. The health care provider will decide the type of urodynamic test based on the person’s health information, physical exam, and LUTS. The urodynamic test results help diagnose the cause and nature of a lower urinary tract problem. Most urodynamic tests do not involve special preparations, though some tests may require a person to make a change in fluid intake or to stop taking certain medications. Depending on the test, a person may be instructed to arrive for testing with a full bladder. What are the urodynamic tests?Urodynamic tests include
UroflowmetryUroflowmetry is the measurement of urine speed and volume. Special equipment automatically measures the amount of urine and the flow rate—how fast the urine comes out. Uroflowmetry equipment includes a device for catching and measuring urine and a computer to record the data. During a uroflowmetry test, the person urinates privately into a special toilet or funnel that has a container for collecting the urine and a scale. The equipment creates a graph that shows changes in flow rate from second to second so the health care provider can see when the flow rate is the highest and how many seconds it takes to get there. Results of this test will be abnormal if the bladder muscles are weak or urine flow is blocked. Another approach to measuring flow rate is to record the time it takes to urinate into a special container that accurately measures the volume of urine. Uroflowmetry measurements are performed in a health care provider’s office; no anesthesia is needed. 
Postvoid Residual MeasurementThis urodynamic test measures the amount of urine left in the bladder after urination. The remaining urine is called the postvoid residual. Postvoid residual can be measured with ultrasound equipment that uses harmless sound waves to create a picture of the bladder. Bladder ultrasounds are performed in a health care provider’s office, radiology center, or hospital by a specially trained technician and interpreted by a doctor, usually a radiologist. Anesthesia is not needed. Postvoid residual can also be measured using a catheter—a thin flexible tube. A health care provider inserts the catheter through the urethra up into the bladder to remove and measure the amount of remaining urine. A postvoid residual of 100 milliliters or more is a sign that the bladder is not emptying completely. Catheter measurements are performed in a health care provider’s office, clinic, or hospital with local anesthesia. Cystometric TestA cystometric test measures how much urine the bladder can hold, how much pressure builds up inside the bladder as it stores urine, and how full it is when the urge to urinate begins. A catheter is used to empty the bladder completely. Then a special, smaller catheter is placed in the bladder. This catheter has a pressure-measuring device called a manometer. Another catheter may be placed in the rectum to record pressure there. Once the bladder is emptied completely, the bladder is filled slowly with warm water. During this time, the person is asked to describe how the bladder feels and indicate when the need to urinate arises. When the urge to urinate occurs, the volume of water and the bladder pressure are recorded. The person may be asked to cough or strain during this procedure to see if the bladder pressure changes. A cystometric test can also identify involuntary bladder contractions. Cystometric tests are performed in a health care provider’s office, clinic, or hospital with local anesthesia. 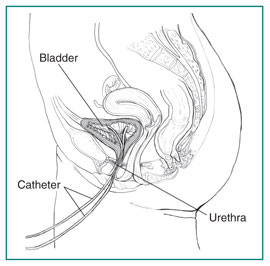
Leak Point Pressure MeasurementThis urodynamic test measures pressure at the point of leakage during a cystometric test. While the bladder is being filled for the cystometric test, it may suddenly contract and squeeze some water out without warning. The manometer measures the pressure inside the bladder when this leakage occurs. This reading may provide information about the kind of bladder problem that exists. The person may be asked to apply abdominal pressure to the bladder by coughing, shifting position, or trying to exhale while holding the nose and mouth. These actions help the health care provider evaluate the sphincters. Pressure Flow StudyA pressure flow study measures the bladder pressure required to urinate and the flow rate a given pressure generates. After the cystometric test, the person empties the bladder, during which time a manometer is used to measure bladder pressure and flow rate. This pressure flow study helps identify bladder outlet blockage that men may experience with prostate enlargement. Bladder outlet blockage is less common in women but can occur with a cystocele or, rarely, after a surgical procedure for urinary incontinence. Pressure flow studies are performed in a health care provider’s office, clinic, or hospital with local anesthesia. ElectromyographyElectromyography uses special sensors to measure the electrical activity of the muscles and nerves in and around the bladder and the sphincters. If the health care provider thinks the urinary problem is related to nerve or muscle damage, the person may be given an electromyography. The sensors are placed on the skin near the urethra and rectum or on a urethral or rectal catheter. Muscle and nerve activity is recorded on a machine. The patterns of the nerve impulses show whether the messages sent to the bladder and sphincters are coordinated correctly. Electromyography is performed by a specially trained technician in a health care provider’s office, outpatient clinic, or hospital. Anesthesia is not needed if sensors are placed on the skin. Local anesthesia is needed if sensors are placed on a urethral or rectal catheter. Video Urodynamic TestsVideo urodynamic tests take pictures and videos of the bladder during filling and emptying. The imaging equipment may use x-rays or ultrasound. If x-ray equipment is used, the bladder will be filled with a special fluid, called contrast medium, that shows up on x-rays. X-rays are performed by an x-ray technician in a health care provider’s office, outpatient facility, or hospital; anesthesia is not needed. If ultrasound equipment is used, the bladder is filled with warm water and harmless sound waves are used to create a picture of the bladder. The pictures and videos show the size and shape of the bladder and help the health care provider understand the problem. Bladder ultrasounds are performed in a health care provider’s office, radiology center, or hospital by a specially trained technician and interpreted by a doctor, usually a radiologist. Although anesthesia is not needed for the ultrasound, local anesthesia is needed to insert the catheter to fill the bladder. What happens after urodynamic tests?After having urodynamic tests, a person may feel mild discomfort for a few hours when urinating. Drinking an 8-ounce glass of water every half-hour for 2 hours may help to reduce the discomfort. The health care provider may recommend taking a warm bath or holding a warm, damp washcloth over the urethral opening to relieve the discomfort. An antibiotic may be prescribed for 1 or 2 days to prevent infection, but not always. People with signs of infection—including pain, chills, or fever—should call their health care provider immediately. How soon will test results be available?Results for simple tests such as cystometry and uroflowmetry are often available immediately after the test. Results of other tests such as electromyography and video urodynamic tests may take a few days to come back. A health care provider will talk with the patient about the results and possible treatments. Points to Remember
Clinical TrialsThe National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions. What are clinical trials, and are they right for you?Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you. What clinical trials are open?Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov. This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts. The NIDDK would like to thank: Syndicated Content Details: Source URL: https://www.niddk.nih.gov/Syndication/urodynamic-testing Source Agency: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Captured Date: 2016-04-26 14:26:00.0
|