
Definition & Facts
What is appendicitis?
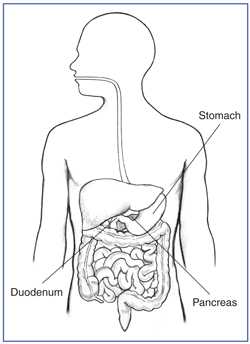
Appendicitis is inflammation of your appendix.
How common is appendicitis?
In the United States, appendicitis is the most common cause of acute abdominal pain requiring surgery. Over 5% of the population develops appendicitis at some point.1
Who is more likely to develop appendicitis?
Appendicitis most commonly occurs in the teens and twenties but may occur at any age.1
What are the complications of appendicitis?
If appendicitis is not treated, it may lead to complications. The complications of a ruptured appendix are
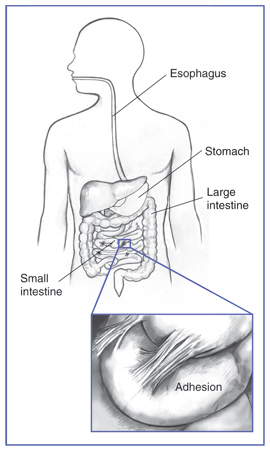
- peritonitis, which can be a dangerous condition. Peritonitis happens if your appendix bursts and infection spreads in your abdomen. If you have peritonitis, you may be very ill and have
- fever
- nausea
- severe tenderness in your abdomen
- vomiting
- an abscess of the appendix called an appendiceal abscess.