










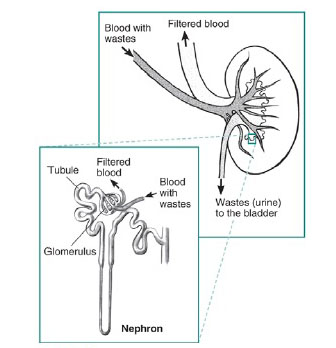








What is PKD?
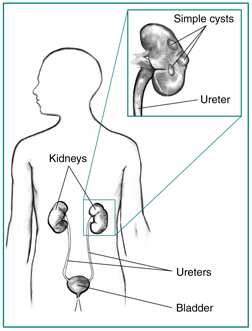
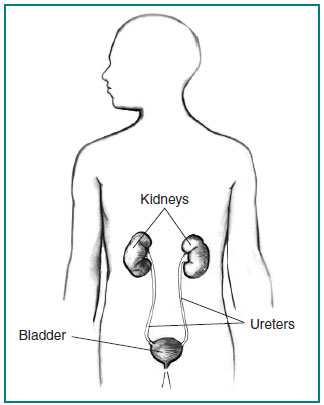
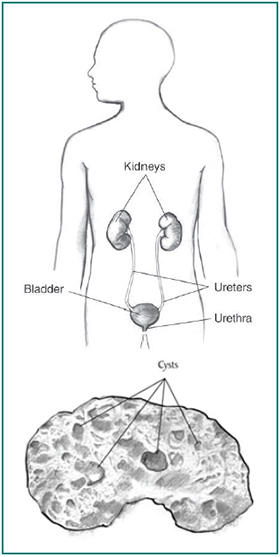
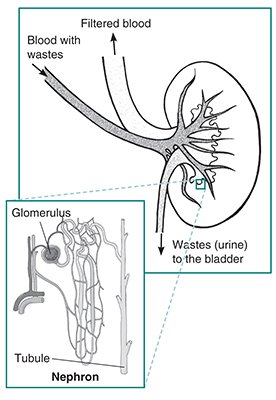
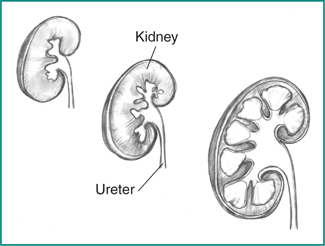
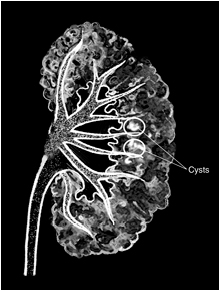
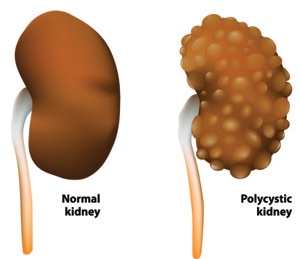
Polycystic kidney disease (PKD) is a genetic disorder that causes many fluid-filled cysts to grow in your kidneys. Unlike the usually harmless simple kidney cysts that can form in the kidneys later in life, PKD cysts can change the shape of your kidneys, including making them much larger.
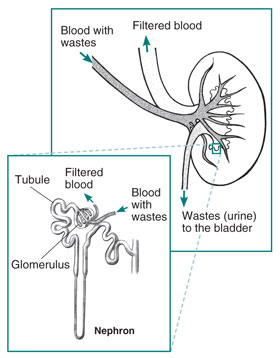
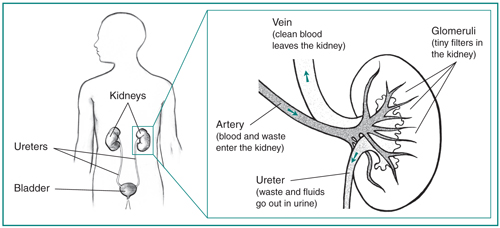
PKD is a form of chronic kidney disease (CKD) that reduces kidney function and may lead to kidney failure. PKD also can cause other complications, or problems, such as high blood pressure, cysts in the liver, and problems with blood vessels in your brain and heart.
What are the types of PKD?
The two main types of PKD are
- autosomal dominant PKD (ADPKD), which is usually diagnosed in adulthood
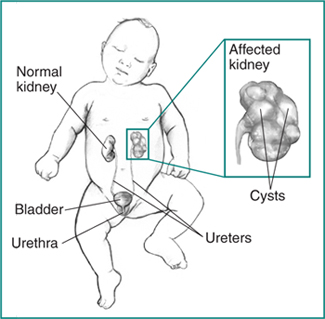
- autosomal recessive PKD (ARPKD), which can be diagnosed in the womb or shortly after a baby is born
How common is PKD?
PKD is one of the most common genetic disorders. PKD affects about 500,000 people in the United States.1
ADPKD affects 1 in every 400 to 1,000 people in the world, and ARPKD affects 1 in 20,000 children.2,3
Who is more likely to have PKD?
PKD affects people of all ages, races, and ethnicities worldwide. The disorder occurs equally in women and men.
What causes PKD?
A gene mutation, or defect, causes PKD. In most PKD cases, a child got the gene mutation from a parent. In a small number of PKD cases, the gene mutation developed on its own, without either parent carrying a copy of the mutated gene. This type of mutation is called “spontaneous.” Read more about genes and genetic conditions.
What are the signs and symptoms of PKD?
The signs and symptoms of ADPKD, such as pain, high blood pressure, and kidney failure, are also PKD complications. In many cases, ADPKD does not cause signs or symptoms until your kidney cysts are a half inch or larger in size.
Early signs of ARPKD in the womb are larger-than-normal kidneys and a smaller-than-average size baby, a condition called growth failure. The early signs of ARPKD are also complications. However, some people with ARPKD do not develop signs or symptoms until later in childhood or even adulthood.
Can I prevent PKD?
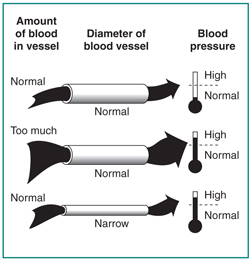
Researchers have not yet found a way to prevent PKD. However, you may be able to slow PKD problems caused by high blood pressure, such as kidney damage. Aim for a blood pressure goal of less than 120/80. Work with a health care team to help manage your or your child’s PKD. The health care team will probably include a general practitioner and a nephrologist, a health care provider specializing in kidney health.
What can I do to slow down PKD?
The sooner you know you or your child has PKD, the sooner you can keep the condition from getting worse. Getting tested if you or your child are at risk for PKD can help you take early action.
You also can take steps to help delay or prevent kidney failure. Healthy lifestyle practices such as being active, reducing stress, and quitting smoking can help.
Make lifestyle changes
Be active for 30 minutes or more on most days. Regular physical activity can help you reduce stress, manage your weight, and control your blood pressure. If you are not active now, ask your health care provider about how much and what type of physical activity is right for you.
If you play contact sports, such as football or hockey, a health care provider should do a magnetic resonance imaging (MRI) test to see whether these sports are safe for you. Trauma to your body, especially to your back and sides, may cause kidney cysts to burst.
Lose weight. Being overweight makes your kidneys work harder. Losing weight helps protect your kidneys.
Aim for 7 to 8 hours of sleep each night. Getting enough sleep is important to your overall physical and mental health and can help you manage your blood pressure and blood glucose, or blood sugar.
Reduce stress. Long-term stress can raise your blood pressure and even lead to depression. Some of the steps you take to manage your PKD are also healthy ways to cope with stress. For example, getting enough physical activity and sleep helps reduce stress.
Quit smoking. Cigarette smoking can raise your blood pressure, making your kidney damage worse. Quitting smoking may help you meet your blood pressure goals, which is good for your kidneys and can lower your chances of having a heart attack or stroke. Quitting smoking is even more important for people with PKD who have aneurysms. An aneurysm is a bulge in the wall of a blood vessel. For tips on quitting, go to Smokefree.gov.

Change what you eat and drink
You may need to change what you eat and drink to help control your blood pressure and protect your kidneys. People with any kind of kidney disease, including PKD, should talk with a dietitian about which foods and drinks to include in their healthy eating plan and which may be harmful. Staying hydrated by drinking the right amount of fluid may help slow PKD’s progress toward kidney failure. Read more about what to eat or drink if you have PKD or are at risk for PKD.
Take blood pressure medicines
If lifestyle and diet changes don’t help control your blood pressure, a health care provider may prescribe one or more blood pressure medicines. Two types of blood pressure medicines, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs), may slow kidney disease and delay kidney failure. The names of these medicines end in –pril or –sartan.