Definition & Facts
What are bladder control problems in children?
Children may have a bladder control problem—also called urinary incontinence (UI)—if they leak urine by accident and are past the age of toilet training. A child may not stay dry during the day, called daytime wetting; or through the night, called bedwetting.
Children normally gain control over their bladders somewhere between ages 2 and 4—each in their own time. Occasional wetting is common even in 4- to 6-year-old children.
By age 4, when most children stay dry during the day, daytime wetting can be very upsetting and embarrassing. By ages 5 or 6, children might have a bedwetting problem if the bed is wet once or twice a week over a few months.
Most bladder control problems disappear naturally as children grow older. When needed, a health care professional can check for conditions that may lead to wetting.
Loss of urine is almost never due to laziness, a strong will, emotional problems, or poor toilet training. Parents and caregivers should always approach this problem with understanding and patience.
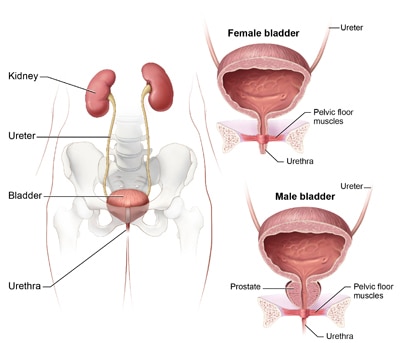
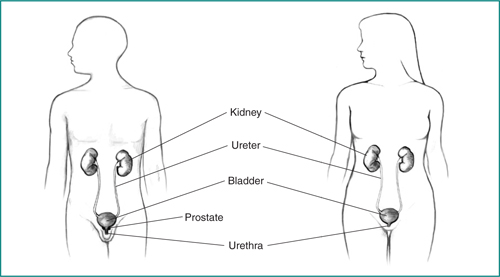
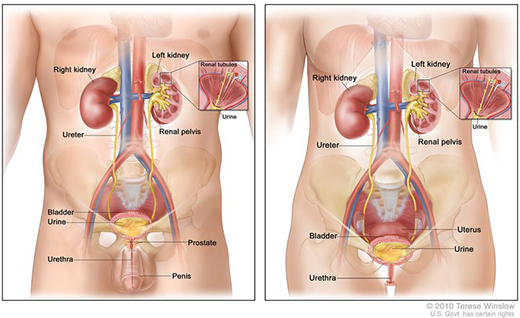
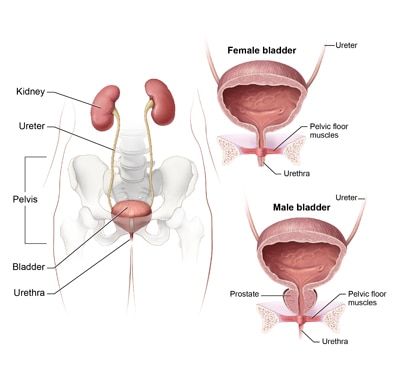
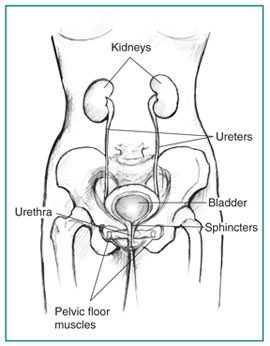
Learn more about the urinary tract and how it works.

Do bladder control problems have another name?
Bladder control problems are also called urinary incontinence or enuresis.
- Primary enuresis is wetting in a child who has never regularly stayed dry.
- Secondary enuresis is wetting that begins after at least 6 months of staying dry.
What are the types of bladder control problems in children?
Children usually have one of two main bladder control problems:
- daytime wetting, also called diurnal enuresis
- bedwetting, also called nocturnal enuresis
Some children may have trouble controlling their bladders both day and night.
Daytime wetting
For infants and toddlers, wetting is a normal part of development. Children gradually learn to control their bladders as they grow older. Problems that can occur during this process and lead to daytime wetting include
- Holding urine too long. Your child’s bladder can overfill and leak urine.
- Overactive bladder. Your child’s bladder squeezes without warning, causing frequent runs for the toilet and wet clothes.
- Underactive bladder. Your child uses the toilet only a few times a day, with little urge to do so. Children may have a weak or interrupted stream of urine.
- Disordered urination. Your child’s bladder muscles and nerves do not work together smoothly. Certain muscles cut off urine flow too soon. Urine left in the bladder may leak.
Bedwetting
Children who wet the bed fall into two groups: those who have never been dry at night, and children who started wetting the bed again after staying dry for 6 months.
How common are bladder control problems in children?
Bladder control problems are common in children. About 1 in 10 children has trouble with daytime wetting at age 5.1 Nighttime wetting is more common than daytime wetting.
| Age2 | Bedwetting Numbers |
|---|---|
| Age 5 | About 1 in 6 children |
| Age 6 | About 1 in 8 children |
| Age 7 | 1 in 10 children |
| Age 15 | 1-2 in 100 children |

Who is more likely to have bladder control problems?
Daytime wetting is more common in girls than boys.
Bedwetting is more common in boys—and in all children whose parents wet the bed when they were young. Your child’s chances of wetting the bed are about 1 in 3 when one parent was affected as a child. If both parents were affected, the chances that your child will wet the bed are 7 in 10.2
Most children with bladder control problems are physically and emotionally normal. Certain health conditions can make a child more likely to experience wetting, including
- a bladder or kidney infection (urinary tract infection)
- constipation—fewer than two bowel movements a week, or bowel movements in which stool is painful or hard to pass
- nerve problems, such those seen with spina bifida, a birth defect
- vesicouretal reflux (VUR), backward flow of urine from the bladder to the kidneys
- diabetes, a condition in which blood glucose, also called blood sugar, is too high
- problems with the structure of the urinary tract, such as a blockage or a narrowed urethra
- obstructive sleep apnea (OSA), a condition in which breathing is interrupted during sleep, often because of inflamed or enlarged tonsils
- ADHD, or attention deficit hyperactivity disorder
What are the complications of bladder control problems?
Children can manage or outgrow most bladder control problems with no lasting health effects. However, accidental wetting can cause emotional distress and poor self-esteem for a child as well as frustration for families.
Bladder control problems can sometimes lead to bladder or kidney infections (UTIs). Bedwetting that is never treated during childhood can last into the teen years and adulthood, causing emotional distress.