|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Motor Vehicle Crash Deaths in Metropolitan Areas — United States, 2009Although rates have declined in recent years, motor vehicle crashes (MVCs) remain a leading cause of injury death in the United States (1). In 2009, a total of 34,485 MVC deaths were reported among U.S. residents, and 22% of those who died were aged 15–24 years. MVCs were the leading cause of death for that age group, which represents approximately 14% of the total U.S. population (1). To assess patterns in MVC death rates for persons of all ages and for those aged 15–24 years, in recognition of the elevated risk for this age group, CDC used data from the National Vital Statistics System (NVSS) and the U.S. Census Bureau for 2009 representing the 50 most populous U.S. metropolitan statistical areas (MSAs). The overall MVC death rate (age-adjusted) for all 50 MSAs combined was 8.2 per 100,000 residents, compared with a national rate of 11.1; among MSAs, rates ranged from 4.4 to 17.8. For persons aged 15–24 years, the MVC death rate was 13.0 per 100,000 residents for all MSAs combined (range: 7.3–25.8), compared with a national rate of 17.3. Although rates for the MSAs generally were lower than the rate for the nation as a whole, higher rates for persons aged 15–24 years were observed both in the MSAs and nationally. The wide variation in rates among MSAs suggests a need to better understand how urban development patterns might relate to MVC deaths and to identify and implement effective strategies to reduce the number of such deaths. NVSS data for the year 2009 were used to identify MVC deaths among U.S. residents (2). Geographic codes indicating county and city of residence were used to tabulate MVC death counts for the 50 largest MSAs (by population rank as of mid-year 2009) and for 63 major cities within these MSAs.* These counts were combined with U.S. Census Bureau population estimates for MSAs and cities to calculate population-based rates for persons of all ages and for those aged 15–24 years. Overall rates (all ages) were age-adjusted to the year 2000 U.S. standard population. MVC death counts <20 (and associated rates) were not reported for MSAs and cities because of concerns regarding statistical reliability and data confidentiality. However, such counts were included in the statistics for all MSAs and all cities combined. The overall MVC death rate for all 50 MSAs combined was 8.2 per 100,000 residents, compared with a national rate of 11.1 (Table). Among the 50 MSAs, rates ranged from 4.4 to 17.8, and 37 (74%) had rates lower than the overall national rate. Rates for MSAs generally were higher in southern states, with the highest rates concentrated in the southeastern United States (Figure). Within the 50 MSAs, the overall MVC death rate for the 63 major cities combined was 7.9 per 100,000 residents. The overall rate for the 53 cities with individually reported data ranged from 3.9 to 19.4. Although the combined rate for the cities was slightly lower than the combined rate for MSAs, 24 (45%) of the 53 cities with individually reported data had higher overall rates than their MSAs. Among persons aged 15–24 years, the MVC death rate for all MSAs combined was 13.0 per 100,000 residents, compared with a national rate of 17.3. Data for this age group were reported individually for 47 of the 50 MSAs; rates ranged from 7.3 to 25.8 and were uniformly higher than the overall (all ages) rates within the respective MSAs. The combined rate for persons aged 15–24 years residing in major cities within these MSAs was 10.9. Rates for this age group were reported individually for only 10 of the 63 major cities, limiting further assessment. Reported byScott R. Kegler, PhD, Office of Statistics and Programming, Laurie F. Beck, MPH, Erin K. Sauber-Schatz, PhD, Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control, CDC. Corresponding contributor: Laurie F. Beck, lbeck@cdc.gov, 770-488-4327. Editorial NoteThe combined overall MVC death rate for the 50 most populous MSAs in the United States was lower than the overall national rate; residents of the MSAs represented 54% of the U.S. population in 2009, while accounting for only 40% of all MVC deaths. In addition, the combined overall MVC death rate for 63 major cities within the MSAs was lower than the combined overall rate for the MSAs. These findings are consistent with statistics showing that MVC death rates are lower in urban areas than in rural areas (3). Although overall MVC death rates in the MSAs generally were lower than the national rate, rates varied widely among MSAs. A similar pattern was observed for MVC death rates among persons aged 15–24 years. In general, rates were higher in MSAs in the southern United States. Urban sprawl, which is a function of residential density, land use mix, presence (or absence) of town centers, and street accessibility (a measure of street density and interconnectedness), might, in part, explain these findings (4). Previous research has shown that sprawl is more common in the southern United States, and that MVC death rates are higher in sprawling metropolitan areas than in compact metropolitan areas (5,6). A growing body of literature examines urban development and its association with MVCs. For example, urban sprawl has been associated with greater driving exposure (i.e., number of miles driven) (4,6). MVCs among teens and young adults (i.e., persons aged 15–24 years) are of particular concern because they represent the leading cause of death in this age group (1). Although MVC death rates for this age group generally were lower in MSAs than for the nation, they nonetheless were routinely higher than overall rates within individual MSAs. For all MSAs combined, the MVC death rate among persons aged 15–24 years was 13.0, which is 59% higher than the combined overall rate for MSAs of 8.2. Well-known risk factors (e.g., inexperience, lack of seat belt use, driving with teen passengers, and alcohol-impaired driving) for teens and young adults likely contributed to the higher MVC death rates observed for this age group. Graduated driver licensing (GDL) programs initially limit teens' independent driving and gradually introduce them to more complex and higher-risk conditions as they gain more experience and move through successive stages (i.e., permit, intermediate/provisional license, and fully unrestricted license) (7). GDL is one evidence-based intervention that can reduce crashes among young drivers, with stronger programs exhibiting greater effect (8). For example, fatal crash rates are lower where GDL programs restrict young drivers from having any passengers than where programs permit one or more passengers (7). Effective interventions to reduce alcohol-impaired driving (e.g., sobriety checkpoints and ignition interlock programs for drivers convicted of alcohol-impaired driving) benefit drivers of all ages, including young drivers who have disproportionately high rates of impaired driving and involvement in alcohol-related fatal MVCs (9,10). The findings in this report are subject to at least four limitations. First, death rates were based on decedent place of residence rather than on place of MVC occurrence; some deaths actually might have resulted from incidents that occurred far away from the city or MSA for which they were reported. Second, MVC death statistics for certain MSAs and cities were not reported because of reliability and confidentiality concerns associated with small counts; for persons aged 15–24 years, data were reported for only 10 of the 63 cities considered. Third, information on risk factors associated with MVC deaths (e.g., nonuse of seat belts, blood alcohol concentration at the time of crash, or vehicle speed) are not included in the NVSS data and therefore, assessing the effects of such factors was not possible. Finally, NVSS data for Ohio, New Jersey, West Virginia, and the District of Columbia showed notable increases for the year 2009 in the number of records with the underlying cause of death coded as "other ill-defined and unspecified causes of mortality," whereas the data for Georgia showed a notable decrease in such records. Although the impact of these changes on MVC statistics is not known, the percentage of such records for each individual state has remained consistently low (=5%). Motor vehicle injury prevention is an important public health priority. The findings in this report indicate that MVC death rates in 2009 varied widely among MSAs, both for residents of all ages and for those aged 15–24 years. Better identification of risk factors related to higher MVC death rates in certain MSAs is needed, followed by implementation of effective strategies for minimizing risks and associated deaths. Proven population-based interventions such as strong graduated driver licensing and alcohol-impaired driving prevention policies offer the potential to further reduce MVC deaths among teens and young adults, the population most at risk for MVCs. References
* An MSA is defined by the U.S. Office of Management and Budget as "a core area containing a substantial population nucleus, together with adjacent communities." What is already known on this topic? Although rates have been declining in recent years, motor vehicle crashes (MVCs) remain a leading cause of injury death in the United States and represent the leading cause of death among teens and young adults nationally. What is added by this report? In 2009, MVC death rates for the 50 most populous U.S. metropolitan statistical areas (MSAs) combined were lower than for the nation overall, for persons of all ages and for those aged 15–24 years. However, MVC death rates varied widely among MSAs, ranging from 4.4 to 17.8 per 100,000 residents of all ages (age-adjusted) and from 7.3 to 25.8 per 100,000 residents aged 15–24 years. In general, rates were higher among MSAs in the southern states. Higher MVC death rates for persons aged 15–24 years were observed both for the MSAs and nationally, compared with rates for persons of all ages. What are the implications for public health practice? The variation in MVC death rates among MSAs suggests a need to better understand the influence of urban development patterns and other factors so that effective strategies can be implemented to reduce MVC deaths. Proven population-based interventions such as strong graduated driver licensing and alcohol-impaired driving prevention policies offer the potential to reduce MVC deaths among teens and young adults.
FIGURE. Motor vehicle crash death rates* for the 50 most populous metropolitan statistical areas — National Vital Statistics System and U.S. Census Bureau, 2009 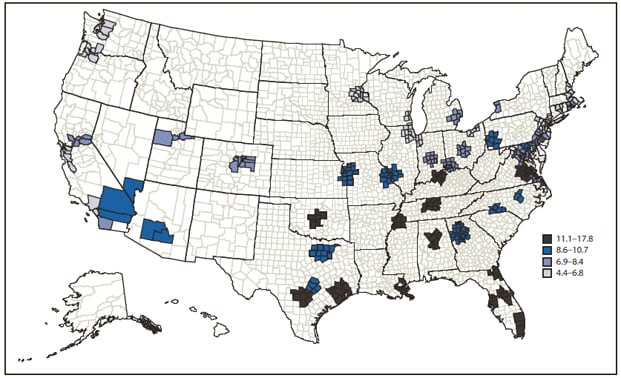
* Per 100,000 population, age-adjusted. Alternate Text: The figure above is a map showing motor vehicle crash (MVC) death rates for the 50 most populous metropolitan statistical areas (MSAs) during 2009, according to the National Vital Statistics System and U.S. Census Bureau. The overall MVC death rate for all 50 MSAs combined was 8.2 per 100,000 residents, compared with a national rate of 11.1. Among the 50 MSAs, rates ranged from 4.4 to 17.8, and 37 (74%) of MSAs had rates lower than the overall national rate. Rates for MSAs generally were higher in southern states, with the highest rates concentrated in the southeastern United States. Syndicated Content Details:
Source URL: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6128a2.htm Source Agency: Centers for Disease Control and Prevention (CDC) Captured Date: 2016-05-23 22:12:05.0
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||